1 Volumes
Sociology: Philadelphia and the Quaker Colonies
The early Philadelphia had many faces, its people were varied and interesting; its history turbulent and of lasting importance.
Indigents
With a long history of welcoming and assisting the poor, Philadelphia has always risked swamping the lifeboat by attracting more of them than it can handle.
Tax Credit Time
 Here's how a discouraging proportion of indigent tax credits go right into the pockets of predators. 
|
| Dr. Fisher |
If we would only listen, most people have a fascinating story to tell. They usually talk quite freely. Take an illustration from the casual observations of an employee of a tax-preparation service. For him, late February to mid-March is "Tax credit time".
Normal behavior for tax-payers is to wait until the last possible moment before the April 15 deadline, not even thinking about unwelcome income taxes. Commercial tax-preparation services have few if any tax-paying customers in March, but are nevertheless extremely busy. The chairs of their waiting area are occupied by citizens, anxious for the government to pay taxes to them as early in the year as possible.
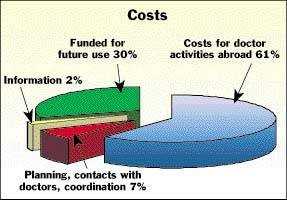
This startling role-reversal is a result of the tax credit system, which should not be confused with tax deductions. In the case of a tax credit, the government issues a check to make up the difference between what the individual earned during a year, and a certain stated income level. No doubt such benevolence is hedged with innumerable rules, restrictions, limitations, and exceptions, which tax preparation services must know all about and, in effect, certify by countersigning the completed tax form. Following that moment, there is a delay of up to three months before the green government check actually arrives. Since a loan against such pending payments is essentially risk-free, the tax preparation service is more than happy to lend it to the recipient. A fairly representative example would be to charge $200 for the preparation service, plus an additional $200 for the three-month loan of, typically, $7000 in tax credits. Where does that lump-sum payment usually go? Almost invariably, it goes to pay down the unpaid balances of credit cards, otherwise running up 18-30% interest, 23% typical. Since David Swensen of Yale's endowment fund is claimed as the world's best investor for achieving a 17% return, the welfare recipients who effectively get 23% by paying off credit cards -- are making a very good investment decision. Indeed, they aren't being swindled out of anything; they come into the tax preparation services loudly demanding just exactly this product. Although they are mainly unwed mothers in their 20s and 30s, they have obviously been well instructed by their friends about how to make quite a shrewd and entirely legal arrangement.
It's only when you ponder the further implications of this whole process that you begin to wonder if there isn't a more efficient way to handle it. Since the underlying security is the full faith and credit of the United States Government, the loan is essentially risk-free. At a time when commercial mortgages are charging about 6%, these loans imply an extra risk premium of at least 15%. If you regard the welfare client as merely a passive intermediary, a $7000 tax credit payment costs the government $1800 of it to deliver only $5200 to the client, net. That is, about a quarter of the cost of the program is going to loan sharks. Surely, a less costly method could be devised to transmit 12 monthly checks to the clients, or even 52 weekly ones.
Beyond that, there is the uncomfortable question of just where we are going with tax credits. Without begrudging a nickel to the poor unfortunates who are helped by this program, it is alarming to hear that low-income housing and historic rehabilitation of old structures are both rewarded with 20% tax credits, and the idea is spreading that it might be a good idea to pay for health insurance with tax credits. We've opened a door here that we may wish we hadn't opened. Echoing the views of Alexis de Tocqueville, Alexander Fraser Tyler has summed it up: "A democracy...can only exist until the voters discover that they can vote themselves money from the Public Treasury."
Winter of Our Discontent

|
| Lyndon Johnson |
In 1965, Lyndon Johnson diverted the (then) rapidly accumulating reserves of Social Security to support his new Medicare program for the sick elderly, along with Medicaid for the sick poor. It was a time of post-war prosperity, the country was sympathetic to the successor to the assassinated John Kennedy, and might well have agreed that the accounting trick Johnson employed was entirely justified. Unfortunately, he was making a huge financial commitment against major political opposition and felt that it was necessary to employ smoke and mirrors to accomplish a worthy goal. His lack of forthrightness however now puts his image in a bad light, when an unexpected demographic event occurred, clearly demonstrating he went beyond his mandate. The totally unforeseen event was that the unusually large generation of baby boomers collectively decided to have fewer children. The "bulge in the python" created the approaching deficit for funding retirements of baby boomers, which the boomers bitterly resent. In spite of that unusually large generation regularly making contributions of 12.4% of income toward providing for its golden years, they now approach the time to spend what they discover really isn't there. President Johnson's accounting trick, called a "unified" budget, was accomplished by describing Medicare and Medicaid as amendments to the Social Security Act. Title 18 was Medicare, Title 19 was Medicaid. Incidentally, those seeking to amend the two medical programs later have thus been destined to be confused for decades by discovering congressional oversight, lies not in the Health committees but in subcommittees of the Ways and Means and Finance Committees. The public shrugged it all off as meaningless congressional quaintness.
A major difference in the way the two medical entitlement programs are financed can if you wish to be similarly traced to quaintness in the former Kerr-Mills and King-Anderson bills, but cynics may imagine more substantial motives. Medicare is entirely a federal program, while Medicaid is nearly half financed by state taxes, while entirely administered by state governments. Federal oversight of the way its share of the money is spent was indeed provided by the enabling legislation. But states have always gone their own way in Medicaid, emitting vast clouds of offended belligerence at the least sign of federal "interference". The central unspoken issue is a recognition that if one state is significantly more generous to the poor than a nearby state, busloads of poor folks might rapidly migrate to take advantage of it. As they migrate in, employers might migrate out rather than pay higher state taxes inevitably generated by new poverty imports. State governments are happy to get the federal Medicaid money, but why must they spend it on poor people?
Whether states express this motive, they have this incentive. Either way, few exceptions are seen to a progressive diversion of federal funds for the hospital and physician costs of the poor, which is what the law intended, into something not intended, payment for nursing homes. In Pennsylvania, for example, less than 2% of the Medicaid budget is now used to reimburse physicians although reimbursement was originally quite adequate. Hospitals now uniformly complain: Medicaid reimbursements have driven away private philanthropy but pay 20% less than the cost of providing care. Indeed, the incentive to provide famous cutting-edge care is blunted for fear of attracting more Medicaid patients who would seek it. Although nursing homes are the main beneficiary of this diversion of funds, they too are funded below a level which would attract out-of-state migrants. This whirlpool of dissatisfaction has evolved during a period of wide-spread surpluses in state budgets. Total funding of the Medicaid program by the federal government is much desired by the states, but likely would not help the poor much; it would help the uninsured. What is most needed here is administrative discipline, and beyond that legislature discipline; an elusive wish since 1790.
State governors have recently taken to urging universal health insurance, but note that insurance is the only industry expressly designated (by the McCarran Ferguson Act) to have state rather than federal regulation. As a consequence, the health insurance industry is deeply intertwined in state politics. The term "Single payer system" is viewed with suspicion by the states as meaning consolidated federal administration, just as the opposite term "Socialized Medicine" alludes to supplanting professional with political control. Patients and doctors use these terms, everyone else is mainly concerned with the money. At 16% of the Gross Domestic Product, it is quite a lot. Naturally, insurance companies deplore that so many people do not own their insurance products, but it is hard to see why anyone else would feel that way.
For example, trial lawyers who even have a candidate for President, seem not to perceive a threat to their business model in total government control of healthcare; they are probably quite wrong. No one in the big industry appears to realize that health costs are progressively narrowing down to the first year of life and the last year; employers have been trapped by a tax abatement into paying for something which in time will scarcely affect their employees. When they do realize it they will surely try to escape their present posture of paying for the whole system with intergenerational transfers. Union leaders do not seem concerned that the coming bankruptcy of Ford and General Motors will probably be blamed on their notoriously generous health insurance benefits. Democratic politicians who were scarcely born when Lyndon fleeced the boomers do not seem to be concerned that the sixties generation loves to make a fuss. Although everyone acknowledges that total coverage leads to higher costs, and higher costs lead to rationing, few people seem to act on this knowledge. Residents of Blue states have scarcely heard of Health Savings Accounts, and if Pete Stark, the current chair of the Health Subcommittee of the House Ways and Means Committee, has his way they never will. But thirteen million people in states colored red on the political map have enrolled in HSAs, in spite of numerous obstacles which Blue politicians placed in their way. No one who wants to pay for drug costs with medical research funds seems to notice that life expectancy in America has increased by nearly twenty years in the same half-century that Russian life expectancy has shortened. Doesn't anyone want a cure for cancer or Alzheimer's Disease?
Have a nice time, suckers.
Old Blockley (P.G.H.)

|
| Old Blockley |
For a long time, the Philadelphia General Hospital was the largest hospital in town, even growing briefly to seven thousand patients during the Civil War, but leveling off at about three thousand at the beginning of the Twentieth Century. At the end of World War II, it had shrunk to about 1500 beds, but it was Medicare and Medicaid in 1965 which finally did it in. By 1977 it was costing the City of Philadelphia about five million dollars a year beyond its revenues to run the place with only 300 patients, while the running expenses of the local private hospitals were actually less, per patient. Titles XVIII(Medicare) and XVIV(Medicaid) of the Social Security act constituted Lyndon Johnson's Great Society, and in effect they made every patient at PGH resemble a walking government check in the mind of hospital administrators. The local hospital association made the argument to the Mayor Rizzo that everybody would be better off if the hospital closed and those government checks were directed to the local voluntary institutions. After a few years, the federal government inevitably squeezed the generosity out of the bargain they would of course now like to abandon. But that's the way it goes. PGH is gone and it isn't coming back. The eighteen acres in Blockley Township, now West Philadelphia, were given to the University of Pennsylvania next door, and gigantic amounts of federal money were contributed to the building of skyscrapers replacements for the original PGH. Ironically, the two hundred children's beds now on the location are fewer in numbers than the three hundred adults once considered too uneconomically few to maintain, and the cost per day of hospitalization is roughly ten times the PGH cost which had been described as unsupportable. The rest of the real estate is built up with buildings involved in medical research, which is also an activity dedicated to working for its own extinction. Discovering a cheap cure for cancer would quickly create a need to fill the vacancies with something else. No one regrets this system of creative destruction, but everyone should regret the diminution of the spirit of local philanthropy which underlay it.
PGH was one of a dozen or so big-city charity hospitals, like Bellevue in New York, Charity in New Orleans, or Cook County Hospital in Chicago. Of these hospitals, PGH had surely been the best, and at the turn of the Twentieth Century a Mayor's commission issued a report about the place which began, "Philadelphia can surely be proud...." Having worked in Bellevue and having visited most of the rest, I can testify that was likely true. When PGH was finally torn down, the walls and floors had such substantial construction that changing the wiring and plumbing to some other purpose had become almost impossible. The PGH nurses were famous for running. Although the alcoholic and drug-addicted patients might be called the dregs of society, the alacrity of the student nurses in running them bedpans or answering other calls, was spectacular to watch. When a doctor came on the floor, they jumped to their feet and were usually ready with the patient's charts, unmasked. Unlike Bellevue, where the floors were creaky and wooden, the open wards at PGH were spacious, clean, well maintained and equipped. At Bellevue, the forty-bed wards were crowded with sixty or seventy patients, so close together you could almost roll from one end of the room to the other without touching the floor. I can remember seeing one seventeen-year-old Bellevue student nurse tending such award at night alone, the intern sharpening needles, and the medical resident developing electrocardiograms in the darkroom. None of this would have seemed acceptable at PGH.
|
| Dr. William Osler |
Old Blockley was the place where modern systems of medical education originated. Up until William Osler came to Philadelphia, medical education mostly consisted of attending eight hours of lectures a day. Osler had an electrifying personality and wandered among the sick at PGH with a train of students following him. He is much quoted, and once suggested his obituary ought to read, "Here lies the man who took the students into the wards." A somewhat more elegant statement of the value of the practical experience was included in his dedication speech at the Boston Library: "To treat patients without books is to sail an uncharted sea. To read books without seeing patients is never to go to sea at all. Osler was somewhat underappreciated during his time in Philadelphia and went on to found the medical school at Johns Hopkins in Baltimore. Nevertheless, the main reason he later left John Hopkins and went to Oxford was his dismay at the adoption of the "full-time" system, which is to say the faculty stopped having a private practice of their own to act as a gold standard for their research and teaching. When all is said and done, there are some areas of discomfort in the transition of students from observers to actors. The PGH system of learning surgery was commonly reduced to a slogan, "See one, do one, teach one,"; things have progressed to the point where it is probably right for the public to insist on greater supervision and control than the old almshouse provided.
The disappearance of old Blockley ended a controversy, or even something of a mystery, about which was the oldest hospital in America, PGH or the Pennsylvania Hospital at 8th and Spruce. There had been an infirmary in Old almshouse at Eleventh Street, and there is no doubt the almshouse was there first. PGH grew out of the almshouse. However, there were many comments at the time of the founding of the Pennsylvania Hospital that it was now the first; that's a strange thing to say when the almshouse was three blocks away. Social historians need to look into the mindset of colonial America, which seems to have included the distinction between the worthy poor and the unworthy poor. Somehow, the founding principal of the Pennsylvania Hospital was to get people back to work who were capable of productive work, possibly even paying for itself in that way. In their minds, apparently just giving solace and help to those who were down and out was not quite the same thing.
Loaves and Fishes

|
| Philadelphia Food Bank |
Philadelphia is full of people and institutions that have done wonderful things without a lot of fanfare and hype, butPhilabundance and its executive director, Bill Clark, surely set some sort of record. The organization has been in existence for twenty years and is generally known as a nice charity that gives surplus food to poor people. And how.
With a four-million dollar budget, they distribute food at a cost of about ten cents a meal. From that, you can easily calculate they are both efficient and big, very big. For a long time, they collected left-over food from restaurants and caterers and gave it to poor folks in shelters. But that was before someone had the brilliant idea to hire an executive director who had formerly been an executive in the supermarket business, rather than a dietician or a social worker or a retired lawyer. Nowadays, Philabundance still takes the calls from restaurants and caterers but refers them to some local food bank to do the pickup. And it doesn't distribute food to the poor itself, instead, it helps new churches get established in poverty regions, showing them how to organize and run food distribution agencies, or stores or kitchens.

|
| Philabundance |
Philabundance is going for big deliveries, and cutting the big costs in the food chain. Clark knew who was dumping the food, by the carload, and it wasn't restaurants. He organized a system of collecting bread from major bakeries, fruit from major importers, meat from the food distribution center -- in carload lots. Someone from inside the food distribution system knows how tightly organized the shelf life is, and if he can get bananas to his eaters in five days, he can have them free from people who absolutely must have eleven days to get them through a delivery chain of fussy people picking and choosing what is on display before they buy. In a market system where food is routinely discarded in order to maintain stable prices (ask any farmer), someone who knows what he is doing can really get some bargains for the poor. You have to know about taxes, too. Donations of food are not just deductible at cost, but at cost plus half of the normal mark-up. A great many of the cargo containers arrive at Philabundance warehouse, unopened because they arrived too late for the weekend buying rush, and would otherwise have to be sold at low Monday prices. There's a lot to learn about this business.
|
| Food stamps |
Food stamps might be a better way to distribute food to the poor, but big cities have an acute shortage of supermarkets, as you soon learn if you live there. New York has an extensive system of neighborhood mom and pop groceries, but Philadelphia doesn't. It's hard to know whether mom and pop stores can't survive in Philadelphia for some reason, or whether New York's notoriously political-legal system is slanted in favor of them, along with rent-controlled apartments on Park Avenue. Supermarkets in center city are hampered by the underlying supermarket the assumption that there will be ample place to park a car at both ends of the shopping trip. Since it is easy to pay $300 a month to park in center city, and even then you find the attendant may have parked someone else in the aisles, you can see that the supermarket idea, which largely developed in Philadelphia in the first place, is more popular in the suburbs.
So, anyway if you are going to throw food away you might as well give it to the poor and get a tax deduction. And if you are going to give food to the poor, you might as well be efficient about it. No doubt there will be some who raise the point that making things free for the poor will attract more of them into the region, raising Medicaid costs and so on. Maybe that's why Bill Clark draws so little attention to the splendid job he is doing, but if so, we really must betray him.
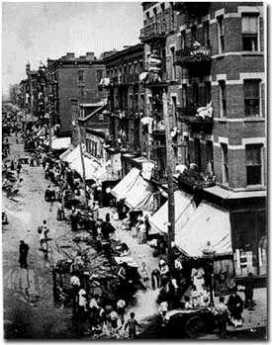
Slum Creation and Urban Sprawl
|
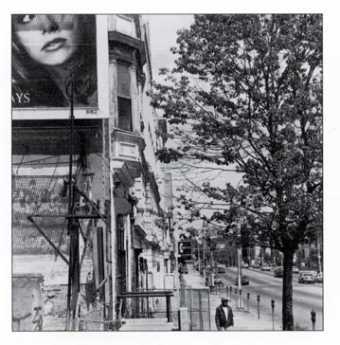
| North Philly |
Slum creation, while occasionally deliberate, is most typically caused by an area's abandonment by previous owners, at lower prices, to bargain hunters. When a large employer moves or closes, the employees seek work elsewhere and sell their houses for what they can get. When the influx of new ethnic groups threatens to weaken real estate prices, panic may be created that waiting too long to sell may find the property worthless; nobody wants to be the last one out the door. During the 20th Century, the driving force in Philadelphia was the flight to the suburbs by people who found a better value in suburban schools, shops, and neighborhoods. All of these processes create slums, almost invariably with a net loss of value in the community. Take a look at those deteriorating mansions on North Broad Street, where the Civil War millionaires used to live. In today's terms, they were once worth several million dollars apiece, but in today's real estate market, they are next to worthless. Value disappeared. The community as a whole is poorer than it was. From the Mayor's point of view, the area has lost its tax base.

|
| New Construction |
Of all these forces, the flight to the suburbs is probably the least destructive to the region, particularly if it is reasonably slow. Out in the suburbs, value is being created as cornfields turn into suburbia, and that added value must be set against the reduced value of the abandoned slum areas. Viewed from the Mayors' perspectives, however, we have a zero sum. The city loses its tax base, the suburbs gain, and local politics soon degenerate into warfare between the suburbs and the city. Not a nice situation, and it cries out for a new civic design. The city politicians have dreamed for a century of city-suburb consolidation, but Philadelphia tried that in 1850. It didn't cure the problem, and it may have created new problems. In any event, suburban politicians live and die on their anti-city rhetoric, and everybody's behavior in the Legislature deserves no kinder description than -- savage.

|
| Orange Station |
Because this issue has been the underlying theme of the Pennsylvania Legislature for two centuries, it repeatedly surfaces in ways that are surprising unless you understand the mechanics of suburban sprawl well enough to see the connection. For example, nowadays a real issue is the three-car family.
During the 19th Century, multi-acre estates spread out along the Main Line of the Pennsylvania Railroad, with the coachman and horses taking plutocrats to the station. Smaller houses, for people who walked to the station, clustered nearby, but you didn't have to go very far from the station to find the gated estates. Suburban development spread out in linear and predictable fashion from the city, along the Main Line. The advent of the automobile freed commuters from the tyranny of railroad station orientation, and middle-class residents could flee the city to areas of the suburbs that were fairly far from the railroad and its stations. But not too far, because there was the problem of the lady of the house, who had to get to the stores. To free her up, the family had to have two cars in the garage. Suburban shopping malls helped her problem, somewhat, but the railroad station was still a magnet.
And then, the majority of married women became working wives, confronting the problem of kids getting to the confounded school. The highly questionable solution of giving the kids a collective car as soon as the oldest got a license, made the oldest kid proudly take the role the coachman used to have, and it caused a lot of teenage turmoil that need not be described here. The point to be stressed is that the three-car family sent home-building into cornfields that were not even close to the main road. Since land gets cheaper the further you get from the city, an economic incentive is created to enter uncongenial social environments, and adopt unexamined attitudes about the environment that are ultimately flatly contradictory.
When the kids leave home, the exurban pioneers no longer need the third car, and think about returning to city life. So far, however, they have been returning to Center City, not the residential neighborhoods they used to call home.
Police Athletic League

|
| pal |
T he Philadelphia chapter of the PAL is now almost sixty years old; that means its origins are to be found in the great industrial migrations and urban dislocations of World War II. Philadelphia has experienced many upsurges of crime in its long history, and almost without exception crime centers in new immigrant groups. Commentators on prison conditions over the centuries have always remarked on the over-representation of whatever is the most recent immigrant group among the inmates. Crimes related to recreational drugs may be an exception, just as crimes related to bootlegging were an exception during Prohibition. Or maybe not; perhaps issues of that sort merely affect the type of crime and the reason for committing it, while the criminals themselves continue to concentrate in the most recent immigrant population. It is merely to face the plain facts to notice that the war industries attracted large immigration to Philadelphia of African-Americans, so the recent-immigrant crime wave centered in them. There's actually hope in that if we keep calm about it. It means that crime can in time be expected to settle down, just as it did after the waves of immigration of Irish, Germans, and Scotch in earlier centuries. This wave of immigrants from the Southern states will surely be assimilated, too. Police records show that most crimes are committed by teenagers, committed between 3 PM and 9 PM. The aim of the Police Athletic League is therefore clear: keep teenagers busy and off the streets between 1 PM and 9 PM. The 27 centers of PAL, with nearly 30,000 participants between age 6 to 18, have a budget of over $2 million a year, all privately donated. The contribution of the City Government is to supply police officers to staff the centers, and that is an unexpectedly important thing to do. One might suppose hostile teenagers would be turned off by the presence of "the man", the stormtrooper of the enemy, and perhaps some are. But the presence of police in every center means that PAL is safe when very little else is safe for lower class teenagers. And of course, it is important for teenagers to learn that cops are people. Lots of cops are nice guys who will help you. Lots of cops used to be members of PAL, themselves. A men's luncheon club to which I belong donates the profits from a weekly lottery to PAL, and consequently, a speaker from the League is sent to thank us by giving a talk once a year. The Police Athletic League is clearly evolving. It started out with only programs in boxing and basketball, rather obvious choices. But now, the example of Tiger Woods has stimulated a great deal of interest in golf, which takes place on the loan of time at five local golf courses. Many famous civic leaders are involved in the governance of this organization, and recently the Lend fest family has been especially generous. You can look forward to a large well equipped PAL center soon, at Luzerne and 12th Streets, based on their generosity. It will have, among other things, squash courts, no less. Squash started out as a game in debtor's prison, but it currently has the image of upper-crust exclusivity. It's important to do things like that. And the activities of PAL have further evolved away from prize-fighting into computer classes. A popular new development has been a mathematics competition. It would go too far to say that PAL has saved a whole generation from living the life of the streets. But it's making progress which is very heartening to see.
Settlement Music School
|
| Jane Adams |
The Settlement Music School has six branches, fifteen thousand current students, an $8 million budget, and three hundred thousand alumni. It tells you something about Philadelphia that an organization this large can exist for 98 years, and yet remain almost invisible. So let's tell a few things about it.
The settlement movement began in England around 1880, and was brought to America by a Quaker lady named Jane Addams. Her most famous settlement was called Hull House, in Chicago. Jane Addams seconded the nomination of Theodore Roosevelt at the Progressive Party convention, and was active in the formation of National Association for the Advancement of Colored People, as well as the American Civil Liberties Union. She was a prominent suffragette, and as a Quaker, it might be expected that she was an outspoken pacifist. Remember, what we are talking about here is music.
|
| tenement districts |
Settlements were what nice upper-class ladies called the tenement districts, and a settlement House was a center for activist women to go help the immigrant groups typically found there. Since there is obviously a lot of difference in what needs to be done to help recent ex-slaves, Italian and Jewish immigrants, and all the different ethnic clusters, the Settlement movement is an archipelago of very different forms of social work. One of the ways to appeal to different groups is through the teaching of music, and the teaching on expensive bulky instruments like pianos is quite naturally shared in a school building. While it is true that a couple of Settlement students are admitted to the musical big time at Curtis Institute every year, only a small proportion of Settlement students go on to musical careers. The three most famous musical alumni of the Philadelphia Settlement Music School were Chubby Checker, who invented a dance called the Twist, Albert Einstein. who played the violin in various chamber groups, and former Mayor Frank Rizzo, who learned to play the clarinet.
The mission of the Settlement School has gradually become the spreading of musical appreciation, especially among "the masses", and it measures its success in the size of its audiences rather than by occupying the center of the stage. This function is readily thrust off on them by the eagerness of public school boards to cut expenses, although the School is scarcely in a financial position to go all the way and assume the role of teaching music classes to 250 public schools. Nevertheless, when financial stringency forces the school board to cut expenses, their choice between a music teacher and a football coach is no choice at all. At that moment, a free-standing music appreciation school ceases to be a competitor and becomes a safety valve. When you hear the Settlement School is in need of money, you are likely being told about stringency in the public school budget.
Although the tuition is quite inexpensive for a music school, the students collectively contribute about half of the annual budget. The rest comes mostly from private charity. You really can't expect cutting edge innovation from school children or endowed charities. But somehow this school leaves you with an impression of big missed opportunity in the truly American forms of music like jazz and folk singing. Symphony orchestra was invented in Vienna and flourishes there, so it has a faintly foreign air to it. It's not completely surprising that both the sponsors and the subjects of Americanization for the Slums are hesitant to promote symphonic role models, while the sponsors at least are a little lost in the world of Rock. Not surprising, but something of a pity.
James A. Michener (1907-1997)
|
| James A. Michener |
James Michener seemed headed for a recognizably Quaker life until show business rearranged his moorings. He was raised as a foundling by Mabel Michener of Doylestown, Pennsylvania, under circumstances that were very plain and poor. Many of his biographers have referred to his boyhood poverty as a defining influence, but they seem to have very little familiarity with Quakers. When the time came, this obviously very bright lad was offered a full scholarship to Swarthmore College, graduated summa cum laude, went on to teach at the George School and Hill Schools after fellowships at the British Museum. And then World War II came along, where he was almost but not exactly a conscientious objector; he enlisted in the Navy with the understanding he would not fight.
While in the Pacific, he had unusual opportunities to see the War from different angles, and wrote little short stories about it. Putting them together, he came back after the War with Tales of the South Pacific. Much of the emphasis was on racial relationships, the Naval Nurse who married a French planter, the upper-class Lieutenant (shades of the Hill School) who had a hopeless affair with a local native girl that was engineered by her ambitious mother, as central characters. Michener himself married a Japanese American, Mari Yoriko Sabusawa, whose family had been interned during the War. There are distinctly Quaker themes running through this story.
And then his book won a Pulitzer Prize, Richard Rodgers and Oscar Hammerstein made it into a Broadway musical hit, then a movie emerged. The simple Quaker life was then struck by the Tsunami of Broadway, Hollywood, show biz and enormous unexpected wealth. Just to imagine this simple Bucks County schoolteacher in the same room with Josh Logan the play doctor is to see the immovable object being tested by the irresistible force. Michener retreated into an impregnable fortress of work. He produced forty books, traveled incessantly, ran for Congress unsuccessfully, and was a member of many national commissions on a remarkably diverse range of topics. Although he lived his life in a simple Doylestown tract house, he gave away more than $100 million to various charities and educational institutions.
In his 91st year, he was on chronic renal dialysis. He finally told the doctors to turn it off.
Stephen Girard and Religion
|
| Girard College |
In 1950, an elderly retired gentleman named Witherbee paid me a visit when I was temporarily covering practice for a doctor in Woodbury, New Jersey, in locum tenens, as we say. His medical problem was easily tended, and we chatted.
He told me that he had attended Harvard Divinity School many years before, and one day was about to graduate as an ordained minister. His family and many other proud families were gathered on folding chairs on the lawn in Cambridge to watch the graduation ceremonies. The graduates were called up one by one, in alphabetic order.
Since Witherbee is at the end of the alphabet, he had a lot of time to think over the significance of what the members of his class were doing. In time, thinking over the personal defects of each classmate who preceded him, he became overwhelmed with a personal question. "How can I tell others how to behave, when I don't know how to behave, myself?"
And so, when his turn came, his name was called out, and he rose in his seat. "I decline to graduate."
The consternation of his family can be imagined, along with the stir in the audience, the astonished face of the Dean, and his own confusion about the uproar he had just caused. But although the die was cast, and the action a final one, it had a surprising outcome. The next day, he received a telegram from the Girard College in Philadelphia, inviting him to be considered for the position of Director of Religious Studies. It seems that Stephen Girard had provided in his will that no ordained minister might set foot within the walls of Girard College, and yet they felt they needed someone to oversee the religious study. Witherbee was perfect: he had the credentials, but he did not have the ordination curse.
And so he happily remained in that capacity for the rest of his employed life.
REFERENCES
| Girard College It's Semi Centennial of Girard College: George P. Rupp ASIN: B000TNER1G | Amazon |
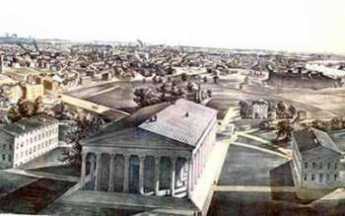
The First and Oldest Hospital in America

|
| South East Prospect of Pennsylvania Hospital |
{kind=link}
There is a painting of the region around 8th and Spruce Streets in the 1750s, depicting a pasture, with cows, and three or four buildings between 8th and 13th Streets. When the Pennsylvania Hospital moved there in 1755 from its temporary location in a house located a block from Independence Hall, there were complaints that it was now located so far out in the woods that it was difficult and dangerous to go there. Still another description of the area is evoked by the provision which the Penn family placed in the deed of gift of the land, strictly forbidding the use of the land as a tannery. Tanneries have always been notorious for giving off noxious odors, so most people wanted them to be somewhere else, anywhere else. In any event, the main activity of Penn's "green country town" at that time was concentrated closer to the Delaware River, and the nation's first hospital was definitely placed in the outskirts. Two blocks further West the almshouse was already in place, but not much else. We are told that Benjamin Franklin had flown his Famous Kite at 9th and Chestnut, using a barn there to store his materials. It might be recalled that the population of Philadelphia, although the second largest English-speaking city in the world, was only about twenty-five thousand inhabitants at the time of the Revolution, and in 1751 was even smaller.
{kind=link}
{kind=link}
In any event, the first and oldest hospital in America was built on 8th Street between Spruce and Pine, and the Eighteenth Century buildings on Pine Street still present a breathtaking view at any season, but particularly in May when the azaleas are in bloom, and fragrance from the flowering magnolias fills the evening atmosphere for blocks around. Although some people today mistake the Pennsylvania Hospital for a state hospital, it was founded in the reign of George II, decades before there was such a thing as the State of Pennsylvania. The Cornerstone was laid by Benjamin Franklin, with full Masonic rites. Most doctors regard a hospital as a mere workshop, but the affection with which many Pennsylvania physicians regarded their special hospital is indicated by the number who have requested that their ashes be buried in the garden.
For two hundred years, beginning with the first American resident physician Jacob Ehrenzeller, the interns and residents were paid no salary, so they had to live on the grounds. An Internet was just that, interned within the four walls for at least two years. Because the resident physicians had no money, they stayed in the hospital at night and on weekends, playing cards and swapping stories. The hospital was home for them, as it was for the student nurses, likewise unpaid but more strictly confined and supervised. This penury seemed acceptable because the patients were mostly charity ward patients, otherwise unable to pay for their own care. Ehrenzeller finished his medical apprenticeship and went to practice for many decades in the farm country of Chester County, but gradually upper-class Philadelphia moved from 4th Street westward to and beyond the hospital, and two of the richest men in American history, Morris and Biddle, had houses within a block of the hospital, although Morris never lived in his house, having more pressing matters in debtor's prison. Therefore, later resident physicians at the hospital had the potential of setting up a private practice in the area and becoming society doctors as well as academically prominent ones. Being a charity hospital in a rich neighborhood created the potential for volunteer work by the town aristocrats and large bequests for charity. The British housed their wounded in the hospital during the Revolutionary War and shot deserters against the red brick wall of the small cemetery to the north. A century later, there were a couple of dozen rooms for private patients in the hospital for the convenience of the doctors and the neighbors, but everyone else was a charity patient. And a century after that, the hospital still did not have an accounting department to collect bills and tended to regard people who asked for a bill as a nuisance. Benjamin Franklin is regarded as the Founder of the hospital, and his autobiography famously describes how he fast-talked the legislature into matching the donations of the public, not mentioning to them that he had already collected enough promises to see the project through. This seems in character; Franklin's biographer Edmond Morgan summed up that, "Franklin doesn't tell us everything, but what he does tell us, is straight." The idea for the hospital was that of Dr. Thomas Bond, whose house is now a bed and breakfast on Second Street, but it was characteristic of Franklin to be the secretary of the first board of managers of the hospital. In Quaker tradition, the clerk of a meeting is the person who really runs the show. It thus comes about that the minutes of the founding board were recorded in Franklin's own handwriting, among them the purpose of the institution, which is to care for the Sick Poor, and if there is room, for Those Who can pay. This tradition and this method of operation continued until the advent in 1965 of Medicare when charity care was displaced by concepts which the nation had decided were better. The Pennsylvania Hospital was not only the first hospital but for many decades it was the only hospital in America. Its traditions, sometimes quaint and sometimes glorious, cast a long shadow on American medicine.
REFERENCES
| America's First Hospital: The Pennsylvania Hospital 1751-1841 William Henry Williams Ph.D. ISBN-10: 0910702020 | Amazon |
Keeping Lunaticks Off the Streets
{kind=link}
|
| Prince Akihito and Elizabeth Gray Vining |
Two Quaker ladies at the AFSC made a totally unique contribution when a request was received to provide a suitable tutor for the Crown Prince, now Emperor. He didn't convert to Christianity, but he later married a Christian, and you can be sure he got a plenty good dose of Quaker style and belief from Elizabeth Gray Vining. This tall, strikingly handsome Philadelphia woman had Bryn Mawr written all over her and turned heads whenever she entered a room. When she went back home, she was followed as a tutor for seven years by, guess who, Esther Rhoads who by then was the director of the Tokyo girls school. It remains to be seen, of course, what the final outcome of this deeply emotional situation will prove to have been. At the moment, the main sufferer seems to be the immensely talented American-educated woman who married the Emperor. But we will see; these are all powerful women in a very quiet way, unaccustomed to losing. One wishes the royal family all the best in their sometimes difficult position.
And then the Service Committee did its work in Vietnam, in Iraq, in Zimbabwe, and Somalia on the unpopular side, in every case. There are stories of venturing into war zones with hundred-dollar bills scotch-taped to their torso, where every fifty feet there was someone who would cut your throat for a dime. One worker in Laos entertained a group of us tourists with tales of living for weeks with nothing to eat but grasshoppers and cockroaches. Dangerous, unpopular, and uncomfortable. It sounds like a wonderful outlet for someone who is a perpetual rebel without a cause, but if you can find one of those at the Service Committee, you must have done a lot of looking.
The Service Committee, like the Quaker school system, is mostly run by non-Quaker staff. That means that neither of them exactly speaks for the religion itself. This little religious group of 12,000 members is stretched thin to provide a vastly greater world influence than its numbers imply. Hidden in the secrets of the group is an enduring ability to attract sincere non-member adherents to their work. And a quiet watchfulness to avoid losing control to any wandering rebels without a cause.
REFERENCES
| Window for the Crown Prince: Akihito of Japan, Elizabeth Gray Vining ISBN-13: 978-0804816045 | Amazon |
Block Captains

|
| Ed Asner |
A block captain is not a ward leader, at least not most of the time. The block leaders of Philadelphia are mostly self-appointed, de facto captains, and yes, they are mostly middle-aged black ladies. Their attitude is that politicians are there to serve the community, not the other way around. At a recent meeting, the leader of the Block Captain's Association called out to the nodding, approving group, "Call your councilman. We elect those people, put 'em to work!"
This enthusiastic group of several hundred grass-roots leaders meets several times a year in, of all places, the hallowed auditorium of the Philadelphia County Medical Society, but doctors are not running this show. Nor is the City Health Department, nor the Department of Streets, nor the various mental health and social service agencies that send representatives. The federal government expressed considerable gratitude in being able to address this group because their new Medicare prescription card was so terribly hard to explain (i.e. it was terribly hard to understand). The genius of the block captain movement is that it appoints leaders to understand what the establishment is trying to say, and then figures out a way to say it. You can make free flu shots available, even take them to the home or workplace, but most people won't accept them unless it is explained by someone they trust. Dead birds don't spread disease, mosquitoes do, but that really sounds a little unlikely. To believe that, you first need the word of a respected local leader. The U.S. Army is built around its sergeants, in the same way. That's in fact how things work at every social level, but in Philadelphia's black communities, it is finally becoming organized. For example, they like pamphlets. Pamphlets are what give sergeants credibility back in the neighborhood.
Success has a thousand fathers, failure is an orphan, so it's now hard to know who started this. Eve Asner, the sister of Ed Asner the movie star, can claim credit for starting a group called Philadelphia More Beautiful, dedicated to cleaning up the messes of the slums, and applying social pressures of a loud and effective sort to irresponsible neighbors. And then, along came the Deputy Health Commissioner Larry Robinson with HEAT. During a hot summer, it was possible for a hundred children and old folks to die of heat prostration because they were confused by dehydration and did things which made matters worse for themselves. The block captains were ideally situated to know who was in danger, who hadn't appeared outside in a day or two, and thus who might need to be forced to drink water or go to an air-conditioned movie. Training the block captains to recognize the signs of trouble fit nicely into the Health Department's ability to measure results with computers. Last year, only seven people died of heat prostration, and everybody knows whose block they lived in.
The Medical Society pays for everybody's lunch at the block captain's meeting, and it is a calculated policy. Every doctor knows how useless it is to talk in terms of calories, carbohydrates, high unsaturated fat content, and water-soluble vitamins. Pamphlets help, but what really works is to serve the block captains a lunch and tell them, now this is what we're talking about. Heaven only knows how that gets translated back in the neighborhood, but surely the first step is to give the block captain an unmistakable message. The Medicare bureaucrat looked visibly relieved when her painfully convoluted explanation of the Medicare prescription card was reduced to about two sentences by questioners in the audience: If you have Medicaid coverage, forget it. If you don't, that card's worth about $600. And this here pamphlet proves I know what I'm talking about.
There did not seem to be a scrap of ideology or power hunger or self-serving -- the usual hallmarks of politics as we commonly observe it. The over-riding principle on which these highly disparate groups are operating together is, pick a problem, and solve it.
Charitable Immunity: An Underestimated Revolution
|
| Percent |
Until 1939, there was a legal doctrine of Charitable Immunity, which universally shielded hospitals and other charitable institutions from negligence lawsuits. No doubt the underlying reasoning was that charities possess limited funds for unlimited demands, and must be forgiven for imperfect compromises in the face of scarcity. To threaten them in court for falling short of perfection might drive charitable efforts away entirely. Since many professionals donated their services to the common effort, there was some spill-over protection for individual professionals, but this centuries-old doctrine applied to institutions more than individuals. There can be little doubt that improved financing of hospitals by health insurance and government programs resulted in both higher standards and lessened public tolerance for imperfection. One might say that twentieth century America decided it could afford better care, supplied the money for it, and expected to see results. It might also be commented that Medicare and Medicaid were significantly overfunded at first, but with time have become painfully underfunded, particularly by Medicaid.
The New Hampshire Supreme Court, against all prevailing doctrine of the time, held in 1939 that hospitals in that state should no longer be broadly shielded from liability by the doctrine of charitable immunity. By 1991, this new legal view had extended to the point where the Pennsylvania Supreme Court felt a need to define Corporate Negligence, emphasizing a hospital's duty to ensure a patient's safety while in the hospital. The court specified the duty to provide safe facilities, to select and retain only competent physicians, to oversee all persons who practice medicine within the walls, and to formulate and enforce adequate rules of behavior. Looking back, legal scholars point to two particularly significant intervening court decisions. In 1957, eight years before Medicare, the New York Court of Appeals declared that to say the doctor is the captain of the ship, acting on his own responsibility, no longer fits the facts. The court bore down hard on the existence of salaried physicians, and the illuminating fact that hospitals were openly sending out bills for medical services. In 1973, the Superior Court of Delaware deliberately and consciously extended the New York doctrine from salaried physicians to independent contractors working within the hospital. But independent contractors are still working for pay; the courts have been more hesitant to extend the idea of corporate control to volunteers who work without payment of any sort. But the movement is in that direction, so it is increasingly difficult to find anyone to volunteer. The American instinct to volunteer is still very great, as the response in 2005 to the South Asian tidal wave demonstrated, with relief agencies forced to send out appeals for the flood of volunteers please to stay home. But the central fact remains that the original premise was limited resources for unlimited needs; Medicare and Medicaid temporarily made it seem resources would be infinite, so why should an injured patient forgive a volunteer. As it becomes increasingly evident that the 1965 federal promises of infinite support are unsustainable, the invalidation of charitable immunity deserves to be re-examined.
The 1973 date of the Delaware decision is probably significant because that was a time of abandonment of malpractice coverage by insurance companies. If you couldn't sue doctors, and you feel you must sue somebody, plaintiffs were in effect told to sue the hospitals. With charitable immunity, hospitals didn't carry insurance, but they immediately searched for it. And thus, a bigger, far juicier deep pocket was created. Physician malpractice premiums, outside of California, were approximately $100 a year. Those rates proved to be far too low. The temporary collapse and disappearance of malpractice insurance companies took place in 1975. It is very hard to blame the actuaries of a malpractice company in say, California, for failing to take fully into account a decision by the Superior Court of Delaware in their premium-setting.
Before this revolutionary upheaval, a volunteer chief of medical staff was (nominally) in charge of every mistake made by any employee, and that was pretty unfair if he got sued. The captain of the ship idea devolved to department heads, or perhaps just the responsible surgeon in the operating room. If the scrub nurse counted sponges wrong and left one behind in the patient, the responsibility passed upward to one of these captains or sub captains. The manifest unfairness of demanding damages from someone six or more steps removed from the incident, particularly one who had a largely honorary title and no real control, exercised a restraint of sorts on lawsuits. Once the blame was shifted to a nebulous legal entity known as the corporation, blameless blame transformed into a corporate financial liability. The average size of awards against institutions escalated upward, raising the size of claims for similar injuries against individual physicians. Add to that the growing fact that hospital revenues are almost exclusively derived from insurance third parties, and thus the premiums for hospital insurance could only come from insurance as an automatic pass-through. Disaster looms if the intermediate parties have nothing to lose, and the public pays all the cost through health insurance or taxes. None of this adversary system, including the whole tort system and the whole malpractice insurance system, was designed to cope with a financially pain-free defense posture. One paradox of the situation is that the admirers of the plaintiff viewpoint are typically also sympathizers with universal health insurance. The two are utterly incompatible under any set of proposals, so far offered.
If matters had stopped at that point, well, it's only money. But obviously, the counter pressure on health insurers to hold down these costs was inevitable. Hospitals were practically under court order to make rules (the hospital associations would be happy to construct a model set of rules) and enforce them on their attending physicians, to pay professionals salaries wherever possible as a time-tested means of encouraging obedience, and to reorganize themselves as corporations practicing medicine rather than hotels providing space and services. (There are legal barriers, of course. Numerous state constitutions awkwardly state "No person may practice medicine in this state without a license so to do.") Needless to say, physicians resisted this trend toward the corporate practice of medicine, even though its early forms only took the shape of placing the hospital lawyer in charge of conferences about "risk" prevention. Since the lawyer knew very little about the topic, the discussion tends to focus on horror stories of suits that were lost or are in litigation.
This struggle between physicians and administrators for control of the hospital, using malpractice as a debating point, is bad enough. Far worse is the slanting of the system of actual medical organization of the staff. Hospitals now often have thousands of nurses and hundreds of doctors, each reporting upward within two guild structures. You would think the chief of surgery would have a lot to say about the selection of the nursing supervisor in the operating room, but heaven forbid. Nurses are hired and fired through the nursing hierarchy, not the department hierarchy which would cross guild lines. It's sometimes hard to say who is on which side of this issue, and probably everybody is on both sides, sufficient to paralyze rational discussion. Everybody involved wants to diffuse blame for an error through the whole organization, and so resists having responsibility conferred in any consistent way. The chief of surgery, for example, is ambivalent about whether he wants nursing errors legally passed back to him, and thus tends to retreat from asserting himself. It can sometimes be hard to specify the ways this chaos expresses itself in poor quality or higher costs, but it would certainly be remarkable if it didn't.
House that Love Built: Ronald McDonald of Philadelphia
Kim Hill had the misfortune to develop leukemia, but the great luck to have Fred Hill of the Philadelphia Eagles football team for a father. Driven by gratitude for the treatment at St. Christopher's Hospital for Children

|
| Audrey Evans |
Fred demanded to be told what he could do and was referred to Dr. Audrey Evans. This world-famous pediatric oncologist was well known for her philanthropic activities and had frequently expressed the need for a temporary residence for families of children needing protracted medical treatments. Young children have young parents, whose savings are soon exhausted by travel, hotel and other non-insured costs related to a seriously sick child. The Hills had just been through such an experience and grasped the problem immediately, adding to it the discomfort and loneliness of families in such a situation. Fred Hill quickly enlisted the enthusiastic support of the whole professional football organization, and Jim Murray the Eagles' general manager recruited Don Tuckerman from their advertising agency, who got to Ed Rensi, the regional manager of McDonald's. Together, they got the project financed and started with a seven-bed facility near Children's Hospital of Philadelphia.

|
| Fred Hall |
In 25 years, the Philadelphia Ronald McDonald House has grown to a capacity of 44 families, in a century-old mansion at 39th and Chestnut Streets filled with Mercer tiles and the like. The operation uses eighteen volunteers at all times, runs two jitney buses, and is one huge teeming family home for people confronting a common issue, supporting each other through a wrenching emotional experience. Although it actually costs about $65 a day per family, the charge is $15 and over half of the clients cannot afford even that. Although an effort is made to have family cooking, the McDonald's restaurant chain supplies 20% of the budget along with generous help with exigencies and in-kind assistance with such things as clowns for the entertainment program, birthdays and the like. Although McDonalds's is probably the world's premier franchising corporation, every one of the 300 worldwide Ronald McDonald Houses is an independent local organization, run without a central headquarters or any sort of standards-setting and the like. Every one of the other 299 Houses got the idea from Philadelphia but proceeds in its own way. Philadelphia created it, but Philadelphia does not own the idea.
In this connection, it is probably worth reflecting on the history of this topic. When Benjamin Franklin and Dr. Thomas Bond started the Pennsylvania Hospital in 1751 at Eighth and Spruce Streets, it was the custom to be diagnosed, treated, be born and to die in your own house. The unique perception behind the nation's first hospital was that poor people generally did not have home facilities that were adequate to support home care. In Franklin's own handwriting the purpose of the Pennsylvania Hospital was stated to be "for the sick poor, and if there is room, for those who can pay." It was understood that poor sick people needed a place to take care of them, not merely for their surgery and overwhelming illness,
<but for convalescence and rehabilitation as well. Two centuries later, in the first thrill of founding the Medicare and Medicaid programs, it was imagined that things would remain exactly the same, only paid for by the Government. But after four or five years, it became abundantly clear that it was far too expensive to use hospitals in that way. The very act of federally paying for the program undermined its volunteer spirit, raised its mandated standards, and made it financially unsustainable. And so, although the 1965 Amendments to the Social Security Act insisted, and still pretend, that no change was to be made to the delivery of care, the delivery of care simply had to be changed. Not only was domiciliary and custodial care to be excluded, but heroic efforts were to be made to reduce the length of stay in the hospital to what would once have been regarded as special intensive care. In effect, if a type of service could normally be handled at home by non-indigent people, it was to be prohibited for everybody. Since the cost of care in hospital has continued to escalate far in excess of the cost of living, it seems unlikely we will ever go back to the days of rest and in-hospital recuperation.
So, just as Dr. Bond recognized the problem and went to Ben Franklin to handle the philanthropy, Dr. Evans had the idea and Fred Hill made it work. Around the Ronald McDonald house, the idea is frequently heard expressed that every hospital needs such a place nearby, for people of all ages. Perhaps that is workable, but it offhand seems more likely that Retirement Villages, so-called CCRC, will be called on to supply this badly needed service, at least for senior citizens. And that what we now call hospitals will evolve into the scientific "focused factories" so popular in the minds at the Harvard Business School.
Slavery: If This be done well, What is done evil?
{kind=link}
|
| Francis Daniel Pastorius |
The Declaration of the German Friends of Germantown, Against Slavery, in 1688.
These are the reasons why we are against the traffic of men's body, as followeth:
Is there any that would be done or handled in this manner? viz.: to be sold or made a slave for all the time of his life? How fearful and faint-hearted are many at sea, when they see a stranger vessel, being afraid it should be a Turk, and they should be taken, and sold for slaves in Turkey. Now, what is this better done, than Turks do? Yea, rather it is worse for them, which say they are Christians; for we hear that the most part of such negers is brought hither against their will and consent and that many of them are stolen. Now though they are black, we cannot conceive there is more liberty to have them, slaves, as [than] it is to have other white ones. There is a saying , that we shall do to all men like as we will be done [to] ourselves; making no difference of what generation, descent, or color they are. And those who steal or rob men, and those who purchase them, are they not all alike? Here is liberty of conscience, which is right and reasonable; here ought to be likewise liberty of the body, except evil-doers, which is another case. But to bring men hither, or to rob, [steal] and sell them against their will, we stand against. In Europe, there are many oppressed for conscience sake; and here there are those oppressed which are of black color. And we who know others, separating wives from their husbands, and giving them to others: and some sell the children of these poor creatures to other men. Ah! do consider well this thing, you who do it, if you would be done in this manner--and if it is done according to Christianity! You surpass Holland and Germany in this thing. This makes an ill report in all those countries of Europe when they hear of [it,] that the Quakers do here handler men as they handle there the cattle. And for that reason, some have no mind or inclination to come hither. And who shall maintain this your cause, or plead for it? Truly, we cannot do so, except you shall inform us better hereof, viz,: That Christians have liberty to practice these things, Pray, what thing in the world can be done worse, towards us, than if men should rob or steal us away, and sell us for slaves to strange countries; separating husbands from their wives and children. Being now this is not done in the manner we would be done at, [by]; therefore, we contradict [oppose], and are against this traffic of men's body. And we who profess that it is not lawful to steal, must, likewise, avoid purchasing such things as are stolen, but rather help to stop this robbing and stealing, if possible. And such men ought to be delivered out of the hands of the robbers, and set free as in Europe. Then is Pennsylvania to have a good report, instead, it hath now a bad one, for this sake, in other countries. Especially whereas the Europeans are desirous to know in what manner the Quakers do rule in their province; and most of them do look upon us with an envious eye. But if this is done well, what shall we say is done evil?
If once these slaves ( which they say are so wicked and stubborn men,) should join themselves--fight for their freedom, and handle their masters and mistresses, as they did handle them before; will these masters and mistresses take the sword at hand and war against these poor slaves, like, as we are able to believe, some will not refuse to do? Or, have these poor negers not as much right to fight for their freedom, as you have to keep them slaves?
Now consider well this thing, if it is good or bad. And in case you find it to be good to handle these blacks in that manner, we desire and require you hereby lovingly, that may inform us herein, which at this time never was done, viz., that Christians have such a liberty to do so. To this end, we shall be satisfied on this point, and satisfy likewise our good friends and acquaintances in our native country, to whom it is a terror, or fearful thing, that men should be handled so in Pennsylvania.
This is from our meeting at Germantown, held ye 18th of the 2nd month, 1668, to be delivered to the monthly meeting at Richard Worrell's.
Garret Henderich
Derick op de Graeff
Francis Daniel Pastorius
Abram op de Graeff.***
At our Monthly meeting, at Dublin, ye 30th 2d mo., 1688, we have inspected ye matter, above mentioned, and considered of it, we find it so weighty that we think it not expedient for us to meddle with it here, but do rather commit it to ye consideration of ye quarterly meeting; ye tenor of it is related to ye truth.On behalf of ye monthly meeting,
Jo. Hart.
***
This above mentioned was read in our quarterly meeting, at Philadelphia, the 4th of ye 4th mo., '88, and was from thence recommended to the yearly meeting, and the above said Derick, and the other two mentioned therein, to present the same to ye above said meetings, it is a thing of too great a weight for this meeting to determine.Signed by order of ye meeting.
Anthony Morris
Insuring the Uninsured is Not Entirely a Health Issue

|
| James Madison |
shrewdly observed that people could and would restrain state taxation by moving to a neighboring state. The founding fathers never contemplated health insurance or Medicaid, of course, but the same principle applies there in reverse. If one state gets too generous with health and welfare benefits, people in neighboring states will nowadays hear of it and get on a bus to relocate advantageously. A flood of new low-income citizens may or may not be what a particular state wants, depending on local economic conditions.
For example during the great depression of the 1930s,

|
| The Great Depression |
Unemployment was so widespread that no state dared attract still more of it with generous welfare benefits. On the other hand, during the recovery period that followed World War II, the industrial northern states definitely did attract cheap labor from the southern states, using better health care, freely available, along with better unemployment benefits. In each case, employers alternate between wanting cheap labor or low taxes, while labor representatives relax or toughen their resistance to the cheap competition. Politicians are always looking for the argument that carries the most votes. If you want to understand the persistence of employer-based health insurance alongside unobtainable health insurance for others, look into this trio of motivations.
While it's true state legislatures must tend to the infrastructure, crime conditions and education, they can in the main be regarded as debating societies between employers and labor. There is some, but not much, the difference between Republicans and Democrats on the Medicaid issue. A Democratic Governor will welcome an influx of low-income voters who will normally vote for his party, but labor unions will soon remind him that enough is enough. A Republican Governor will gladly supply cheap labor for the state's employers until rising taxes bring an end to his support. Since the financial stability of the local hospital can be badly jarred by the instability of Medicaid payments, doctors soon get annoyed with the misalignment between state motives and the welfare of their patients. It is not much of an exaggeration, that state coffers might be overflowing with the surplus, but the budget of Medicaid will not rise a penny if it would attract poverty migrants from neighboring states during a period of high unemployment.
The obvious solution is a federal one, imposing uniform standards. But think that over a little before you jump at it. If the federal government pays all of Medicaid costs, it is going to want to administer the program. All states resist that idea, more so if local and federal political domination is in conflict. Small states will universally be fearful of being overwhelmed by large neighbors, particularly when they have achieved advantageous niches. The disastrous condition of the auto industry might persuade Michigan to agree, but Tennessee and other states with Japanese car plants might disagree. As you get close to the border of large states, hospitals near the border can often attract many patients from the other state; strange political bedfellows can link arms in Congress when you might not expect it.
None of this, absolutely none of it, has to do directly with medical care. But the quality of health care is strongly affected, and doctors are sick of hearing about poor sick folks when the real issue is labor availability. The voice is Jacob's voice, but the hand -- is the hand of Esau.
Unequal Health in an Unequal World
 |
| Sir Michael Marmont |
In 2007, the Sonia Isard Lecture was delivered at the College of Physicians of Philadelphia by Professor Sir Michael Marmot on the topic of Health in an Unequal World . Sir Michael is the Director of the International Institute for Science and Health, and MRC Research Professor of Epidemiology and Public Health, at University College, London.
His starting point is the commonly accepted view that the richer you are, the better your health. The life expectancy of the poorest level of society is almost everywhere seen to be shorter than the local average. In less developed countries and in children, the excess mortality is concentrated in infectious diseases. However, in more affluent nations, it is obesity, diabetes, hypertension which seems to account for it. Regardless of the cause, the common denominator everywhere is poverty, which leads to a general opinion that the alleviation of poverty contains the solution to the health gradient. There is even another logical presumption, that improved health care will directly remedy the problem, without necessarily addressing a more daunting obstacle, the elimination of poverty. Although the provision of equal access to quality health care may be almost more than we can accomplish, in this analysis of causes, it is a short-cut.
Sir Michael is not so sure. Great Britain has had a national health service for fifty years, but it is still clear to British physicians that the class distinction persists in health if not in health care. Mortality statistics confirm the professional opinion. The conclusion is general that the British health system must be flawed, or underfunded, or poorly run. Not necessarily correct, not necessarily correct. Buried in a mountain of data from the Whitehall Studies of British civil servants, Dr. Marmot teased out the fact that a striking inverse gradient of mortality and morbidity existed in a highly educated group that had essentially equal health care and, while not rich were certainly not poor. The gradient persisted at all levels; the higher you rose in the bureaucracy, the longer you were destined to live after retirement.
Evidently a huge amount of statistical work followed this insight, confirming its thesis in a wide variety of situations. The caste system in India provided a confirming example that was unrelated to education or occupational strivings. Marmot's observation is a gradual gradient, not a two-part, either/or. Not rich versus poor, but richer versus less-rich, less-rich versus even-less rich. Every occupational, social or financial step up makes you live a little longer.
I wish he had stopped there. But the pressure to explain has generated the hypothesis that what we are looking at maybe progressive degrees of empowerment. Others who have contemplated Professor Marmot's observations suggest it is due to progressive degrees of happiness. Sorry, but that's a little too touchy-feely for me. I don't know what empowerment is, or how to measure happiness. The monk in his cell may have achieved serenity, not necessarily happiness, certainly not empowerment. The prisoner in his cell has no serenity, happiness or empowerment. I prefer to believe it is premature to speculate publicly about the mechanisms which produce these observations.
Meanwhile, it seems to be true that if you aspire to be rich you may not become happy, but you will probably live longer. If you want to rise in the hierarchy and still live longer, you need not be afraid to strive. For at least a little while longer, that's going to have to suffice as a definition of wisdom.
Community Volunteers in Medicine

|
| Comm Volu In Medicine |
Mary Wirshup has a very different medical background from mine, but she's my kind of doctor. I couldn't help wishing, as she addressed our urban luncheon club, there could be thousands more like her, even while understanding more fully than she seems to, the reasons why doctors are driven from her behavior model. As we parted, it felt like saying a last goodbye to the Spartans marching to Thermopylae.
As 46,000 medically uninsured persons in Chester County get sickness and injuries, they know that a Federal Law prohibits a hospital accident room from refusing to see them, so ways are found to shunt patients to the CVIM free clinic, run by volunteers. This law is, in turn, a response to a government-created situation where a hospital which "accepts" patients must keep them. Any economics teacher can tell you that supply/demand issues are best addressed by price adjustment, so price controls in whatever guise lead to shortages. I must say I have little sympathy with the devious strategies which hospitals often employ to disguise their rejection of uninsured patients. At the same time, I know a lifeboat will sink if too many climbs aboard. Nevertheless, the semantic switch from lack of insurance to lack of care implies that only more insurance can surmount the barriers to care, which is absurd. For one thing, I know too many hospital administrators who are paid a million dollars a year, and one who is paid two million. And at least two health insurance executives are in the newspapers with a net worth over a billion -- yes, that's billion with a b. We have reached a point where reducing all physician income to zero would only reduce "healthcare" costs by 10%. As I look at Dr. Wirshup's modest clothing I can only surmise she plans to continue her modest living until she is 80 years old, after which her savings might see her out. Squeezing physician reimbursement is not intended to save significant money, nor intended to restore physician incomes to more equitable levels. It is intended to address the oversupply of physicians without confronting either the universities or the foreign trained lobby.
The elite tranche of medical schools do their part to relieve physician oversupply without reducing class size, through the encouragement of their students to go into research. I was well along at the National Institutes of Health before I finally decided I had not gone into medical school with that goal, and returned to teaching and patient care in a more satisfying model not too different from CVIM's obviously Pennsylvania Dutch spirit. The Amish at the far western end of Chester County reject the whole idea of insurance; their most characteristic statement is "Don't send me no bills." That attitude is rather a contrast with the shiny housing and automobiles in the Silicon Valley developments of Southern Chester County, or even with some rather bewildered Quaker farm families scattered over the rest of the county next to the horsey set. Chester County is America.
On Second Street in Society Hill, next to the park where William Penn's house stood and a few feet from Bookbinders, is the house of Dr. Thomas Bond. Bond conceived the idea of building the first hospital in America and with Franklin's publicity machine succeeded in getting it built, to care for the "sick poor". Dr. Bond started a second enduring tradition as well. When the Legislature expressed doubt that the institution was sustainable, he pledged to convince the local medical profession to serve the poor without charge. Some of the legislators who voted for the measure did so in the belief that charity care would never appear so the gesture would be without cost. The physicians did indeed come forward, in sufficient numbers to run many institutions for two hundred years. In 1965 health insurance made its national appearance and has regarded the benchmark low costs of charity care as a threat, ever since.
No Laborer Left Behind
 |
| Ivy League |
The top thirty American colleges have ten times the applicants they have room for. Demand vastly exceeds supply, prices are essentially fixed; shortages result. Can-do is the American way, so our first reaction is to build a lot more colleges and beat them over the head if they aren't first-rate. To bring this down to a local scale, implications are that Philadelphia has a moral duty to build eighteen more Ivy-League universities.
 |
| Cosa Ricians Roofers |
Let's think about that, in a back-of-the envelope way. Since the rest of the country is going to be similarly driven, we can't attract Americans to run those universities. Philadelphians who are doing other things must staff those universities; people inclined to become professionals of a different sort are going to have to be trained to be university professors. Students now being rejected will be admitted, since that's the purpose of the thing. Unless we somehow increase academic productivity, every man, woman and child from Trenton to Wilmington is going to be in a college classroom in some capacity or other. We here confront the extrapolation fallacy; a new problem must be addressed in more productive ways than just more of the same.
Curiously, the readjustments to this overall shift from an industrial to a service economy are first making their appearance in things like roof repairs and ironing shirts. When my house needed a new roof, I found I had a choice of workgangs composed of Costa Rican, Puerto Rican, or Polish roofers. The Costa Ricans made the best bid and went to work immediately. They started pounding on my roof at 6 AM, and we're still pounding after I went to bed at night; I have grave doubts that American roofers would approach that work standard. I am told that the entire building industry, on which our current prosperity rests, would collapse if we banned illegal immigration. In a different industry, Philadelphia's convention hall cannot attract visitors unless we build more hotels. But the hotel industry cannot find nearly enough people who speak English to make the beds. For one purpose or another, we have imported 12 million illegal immigrants who mostly remain invisible because they are so hard at work.
We are going too recklessly fast with what is fundamentally a useful transformation of our society. Americans want to go to college because statistics show that will make them prosper. But that's only half of their transformation. The other half is a resulting shortage of labor in the jobs which do not require college. Normally, you would expect wages to rise, but they are suppressed -- deflated -- by substituting immigrant labor, legal and illegal. Impose an effective barrier to immigrants, and you would quickly see inflation like you wouldn't believe. Combat inflation by raising interest rates and the housing market would quickly collapse. That would prove to be a painful way to make the immigrants decide to go back home, although it would be effective. And so on, and so on, and so on.
Slow down, America. You're going in the right direction, but exceeding the speed limit.
Pennsylvania Prison Society

|
| Duke of York |
William Penn, who spent considerable time in British prisons, established a penal code for his new colony which largely swept away the draconian punishments established by the code of the Duke of York. Until as late as 1780, jails were mainly confinement hotels for debtors, prisoners awaiting trial, and witnesses. For actual punishment, the methods were execution and flogging. Penn's Code for Pennsylvania restricted execution to the crime of murder, and flogging to sexual offenses; everything else was punished by fines and imprisonment. Hidden in this code, of course, was the need to invent and construct prisons to service the imprisonment. It would take over a century to address this need, and Philadelphia still has not completely caught up with the need for more prison cells. Without a prison system, the Penn code was impractical, and the colonial penal code retrogressed toward floggings, pillories, and hangings after Penn's death.
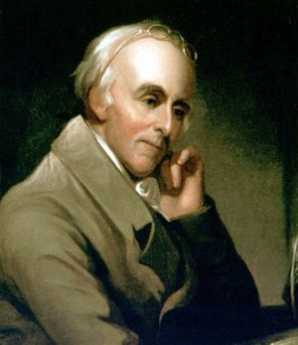
|
| Dr. Benjamin Rush |
In colonial Philadelphia, the main prison was on Walnut Street, with sixteen cells. A neighboring Quaker, Richard Wistar, started a soup kitchen in his own home, taking the soup over to prisoners. By 1773, he had established the Pennsylvania Society for Assisting Distressed Prisoners, which was unfortunately disbanded by the occupying British Army in 1777. In 1783, Dr. Benjamin Rush with the assistance of Benjamin Franklin, Bishop White, and the Vaux family, founded the Philadelphia Society for Alleviating the Miseries of Public Prisons, which after a century changed its name to the Pennsylvania Prison Society. The Prison Society believes it is the oldest continuous non-profit society in America.

|
| Eastern State Penitentiary |
The Prison Society has had several major changes in direction. The original concept was to substitute public labor for imprisonment, a less costly arrangement than imprisonment while avoiding a return to floggings and dismemberment. However, the degrading sight of prisoners in chain gangs caused a public outcry, and the approach was abandoned. In the spirit of the French and American revolutions, loss of liberty was seen as the greatest punishment conceivable. Added to this was the Quaker concept of inspiring remorse through silent meditation, and the eventual outcome was the construction of the Eastern State Penitentiary on what was then called Cherry Hill. In 1823, it was ominous that Eastern State Penitentiary was the largest structure in America. Although the concept was widely admired and imitated, the prolix Charles Dickens took a violent dislike to the idea of never talking to anyone, and led a reversion away from penitentiaries back to simple prisons. In the days before Alzheimers and schizophrenia were well characterized, the spectacle of massive recidivism was added to the rumor that protracted solitude led to insanity.

|
| Catherine Wise |
From Catherine Wise the Communications Director of the Pennsylvania Prison Society, the Right Angle Club recently learned that the current evolution of the American penal system has led to a steady state, but a troubled one. There are 2.2 million inmates in American prisons today, more than any other nation including Russia and China. Of these, 75,000 are confined in Pennsylvania, 9,000 in Philadelphia. Recidivism is 67%, the cost is $31,000 per year per inmate, the majority of inmates have been involved with illicit drugs, a growing number are infected with HIV and Hepatitis C, mental illness runs around 20%. The cost of incarceration is growing faster than the cost of either education or healthcare for the community. Prison overcrowding is extremely serious, the programs for managing parole and integration back into society are weak and underfunded. Eighty percent of the inmates are non-white, most prisons are located in remote regions too far for easy visiting, medical care in prison would not seem at all acceptable in general society. The Prison Society has no difficulty finding projects which are urgently needed. Just for an example, take the peculiar prison statistics; it really seems improbable that only 9,000 of the 75,000 Pennsylvania prisoners are in Philadelphia. Then reflect, NIMBY, that no one wants a prison or its visitors near his home, except areas of rural poverty welcome the employment a prison brings. Reflect for a moment that "jails" are paid for by local county taxes and contain prisoners with less than two years to serve. "Prisons" are paid for with state taxes, and contain those sentenced to longer than two years. Finally, add the fact that nonvoting Philadelphia prisoners in rural prisons are counted by the census as residents of the rural area for the purpose of distributing legislative and congressional seats. The rural politicians love the system, the urban neighbors love to be rid of the prison environment, but the prisoner families can't visit the prisoner. Who cares? Who even notices?
During the first World War, Quaker interest in prison matters was greatly stimulated by the imprisonment of many Quaker conscientious objectors to the wartime draft; since that time prison conditions have again become a central interest of the religion. It's hard to prove but is confidently asserted, that violence and mistreatment of prisoners are appreciably less in Pennsylvania than the rest of the country, California for example. In any event, The Pennsylvania Prison Society is a particularly effective advocate for humane treatment because of credibility achieved over two centuries, with newspaper editors on its board, and sympathetic affiliations with the legislative judicial committees. It knows what it is talking about, as a result of over 5000 annual prison visitations, and it has served the prison administrative corps by performing volunteer work, accepting contracts for parole projects, arranging bus trips for prisoner families to remote prisons, and working for improved funding for prisons. At the moment, there are six highly imaginative bills before the Pennsylvania Legislature, devised and researched by this outside organization with credibility, and political clout. Although the Society takes an occasional contract for a project, it is itself entirely funded by outside contributions, and because of occasional adversarial situations, asks for no funds from the state. Even the contract funds have been questioned, and are only accepted when the working relationships fostered are more useful for the prisoner clients than any co-option which might result.
One final word about medical care in prison. It's not as good as medical care for non-prisoners, and unfortunately it probably never can be. The remote rural location of prisons makes it difficult to obtain physicians and nurses, regardless of wage levels. It's dangerous to be around prisoners, as any guard will tell you, and it's more dangerous to be in control of narcotics amidst a population of addicted convicts. Malingering is nearly universal, both to obtain desired drugs and to spend "easy time" in the infirmary. Many prison escapes are engineered around the necessarily weakened security of the medical system. The prison budgeting system has all the rigidity and weaknesses of any governmental medical system, and in this case, it's run far out of sight of the public. Even the bureaucrats in charge are victimized by other bureaucrats. The average duration of incarceration in Pennsylvania is longer than in most other states; the prisons have to keep mental patients because the mental hospitals have all been closed. Fifty years ago, when there was no place to put a non-criminal with tuberculosis, he was put in jail. The parole system is underfunded, there is not nearly enough community support to absorb ex-con. Behind all this is a shortage of prison facilities. The legislature has got itself into a position that if it moved more prisoners into the outside, more prisoners would just fill the vacancies, costs would go up, and things wouldn't look much better. Only after the backlogs have been absorbed, would there be much visible effect.
Picking Up the Usual Suspects
The federal government directly controls about half of health care spending and makes rules affecting most of the rest.

|
| Claude Rain |
Every group or business which receives some of this money is alert not to lose it. Many other groups are alert for openings to get more of it. All employ sentries in Washington. False alarms are frequent, stealth attacks are a constant threat, constituents paying the bills demand immediate reassurances. Members of Congress seldom initiate a disturbance unless someone from inside an industry brings it to them. Consequently, when proposals do surface and seem to be serious, the question to be immediately answered is -- who's behind this? If you know who starts something, you can readily imagine the motive, assess the political strength, decide how to respond. With what little was generally known about the Clinton Health Care Plan of 1993, it was easy to imagine a host of people with some motive, but very hard to say who was actually pushing one. Must be a Democrat, obviously, but not immediately obvious which of several possibilities was the real agitator.
Health insurance companies would always seem likely to have proposals about national health insurance. Blue Cross dominates the market in large geographical markets, mainly East Coast, and would seem fearful to lose that dominance in a major upheaval. But other market areas of the country are dominated by commercial insurance companies who might seek to upend the Blue Cross monopoly, but whose form of business would be even more seriously threatened by health insurance innovations. Most commercial health insurance was written by large life insurance companies who regard health insurance as a small sideline for the convenience of their industrial customers. Blue Cross was somewhat more comfortable with government work, particularly since the 1965 Medicare and Medicaid programs were patterned after them. However, Blue Cross was non-profit, thus lacking in incentives, and historically controlled by health care providers. That is, Blue Cross was formed by and dominated by the hospital associations, and Blue Shield was formed by and dominated by medical societies. Since doctors and hospitals were very prompt in announcing their deep concerns and uncertainties about the Clinton Plan, Blue Organizations seemed unlikely to make daring proposals so likely to provoke trouble at home.
Not that some doctors and some hospitals didn't try to see what might be made of this opportunity. At the American Medical Association, certain leaders known to have Blue Shield involvement offered conciliatory remarks about waiting for further details before taking a stance but were abruptly halted by a general opinion that things had apparently already gone too far for substantive negotiation. Much the same thing occurred at the Hospital Association; the winners had too much to lose, the losers had too little influence to matter, and nobody stepped up to claim an inside track. Hospital trustees didn't know what was going on, strongly suspected something was going on and didn't like either situation. If the doctors got mad enough at a hospital, they could ruin it, and if hospitals got mad enough at Blue Cross, it too was ruined. The main strength behind the Blue Cross monopoly position was the secret discount provided to them by hospitals, which was refused to competitor insurance companies but could easily be extended in the interest of fairness. If need be. The commercial competitors wanted that discount much more than they wanted new insurance models.
There is one subset of doctors and hospitals that might be suspected of generating a sweeping revision of the medical system -- academia. Medical schools think of themselves as the appropriate source of vision about the profession they are training, and they run large prestigious hospitals. Their heavy dependence on government research grants, teaching subsidies, and tuition support programs puts them in constant contact with Washington bureaucracy and politics; propinquity is a great match-maker. Their style of salaried faculty creates estrangement from making a living by being paid fees for specified services, and they are reasonably comfortable with the flaws and techniques of professional promotion within a large organization. So, a slogan which has been attributed to Wilbur Cohen himself does not greatly jar on their ears. The author of the Medicare Act is said to have announced that the entire medical system of America could be accommodated by thirty or forty Mayo Clinics. Twist that just a little, and you are imagining he said forty or fifty medical school teaching hospitals. The briefest contemplation and rebuttal will knock down that proposal, such as pointing out that we have several times that many teaching hospitals at present without achieving anything like the nation-wide coverage envisioned. After absorbing the administrative chaos of readjusting to that model, you would confront the old repeated history of grossly overestimating, and then grossly underestimating, the future manpower needs of a medical system in the process of constant scientific turmoil. Suppose you built the fifty Mayo Clinics and found you needed two hundred? Suppose you built two hundred and found you needed seventy? And then, finally, remember that each big city could expect to contain one of these organizations, but the fewer of them there are, the longer the distance everyone else would have to travel to get to them. No one has even ventured to speculate how you could go about doing such a thing, let alone doing it three or four times to get it right. But, but. The infeasibility of academia at the center of medical care delivery does not eliminate the possibility that the idea underlying the Clinton Health Plan may have originated in academia, or that academia might support some similar proposal with something else at its center.
Since it was soon clear that the traditional "players" in the health policy arena were unlikely to be sponsoring some self-serving policy that might masquerade as the Clinton Health Plan, the search went on. There were a number of professional groups within the medical community who had traditionally chafed at the domination of the hierarchy by physician leadership. Nurses, hospital administrators, pharmaceutical companies, druggists, corporate human resources officers, public health officials, social workers, biology teachers all represented groups who derived status with the public by displaying inside knowledge of medicine. But all of them fell silent when a physician entered the room, and tended to shift their emphasis to faults of the "system" or the "industry". Their Washington representatives placed their emphasis on changes in the existing system which might elevate the prestige and income of the members and were particularly vigilant for system modifications intended for other purposes which might nevertheless create advantageous loopholes for the members. All of this is normal striving in the good ole' American way, a polite variant of the mixture of bellicosity and restraint usually seen in the Union movement. These people wanted to improve their income and working conditions but were ultimately quite hesitant about radical proposals that might sink the ship. A quick survey showed they were not supporting any particular reform project, even though they could be counted on to support any reform project. Furthermore, they consistently injured their political strength by extending beyond economic goals to issues like radical feminism in the case of nurses, or direct advertising to the public as in the case of the drug companies, or practicing medicine without a license in the case of limited-license practitioners. These people had votes, influence, and lobbyists, but they did not have a national project for health care reform of their own devising, and they surely were not the people behind the Clinton Plan.
During the six months before The Plan was presented to Congress and the Public, a White House task force said to consist of five hundred secret members was meeting under the direction of President Clinton's wife Hillary. No doubt part of their purpose was to give Hillary a public platform on which to show her stuff, with the idea of someday succeeding her husband as President sort of in the back of her mind. But most of it was also quite practical; somebody had to figure out what this proposal was going to be, and newly elected Bill had to spend most of his time learning how to run the rest of the country. Buried in here was an efficiency principle too; the staff members of every important congressman and senator were involved in the process, making the deals and surfacing the political angles before things had to come down to votes and filibusters. Meanwhile, the rest of the country had to wait outside closed doors, fed by rumors and spin.
How well I remember one public seminar on the subject during this period of suspense. The audience was filled with people thought to be influential with the public, the usual suspects in that sense, too. Representatives of various interest groups were seated up front at a table, and for some reason, I had been picked to represent doctors. Next to me was a druggist who had made a billion dollars starting an HMO; it was intriguing to watch how many well-dressed women with no interest in health care paraded up to the table to show their stuff to the billionaire, while we waited for the meeting to begin. All of the usual suspects of Philadelphia medical care were at the table, each of us wondering what the other was going to say. When some last Very Important Person had wandered in and taken a seat, it was time to begin. The moderator told a funny story or two, and then asked each one of us what we thought of the Clinton Health Plan. One by one, to the utter amazement of us all, we each explained how we were opposed to it.
So obviously this proposal was not coming from the usual agitators. But, remember, somebody was surely behind it. Before we take a stab at that mystery, let's humanize the usual suspects by describing a few of them.
Health Maintenance Organizations (HMO)

|
| HMO |
It's an ancient wrangle whether a manufacturer should actually own its suppliers or the reverse; or instead whether it's healthier for industry components to stand at arm's length from each other. At issue is not only what is best, but what is fair. If industry mergers seem sufficiently unfair, it will be proposed they should be illegal. That's the main substance of a lot of antitrust argument. Unfortunately, what is valid in good times may be reversed in a downturn. A prosperous supplier of materials often acts as a "cash cow", saving a merged enterprise from bankruptcy. Unfortunately, within a different economic climate one badly failing supplier can bring down the whole merged enterprise. There's also organizational friction; a temporarily prosperous unit may get to thinking it should boss the less prosperous units around. At the very least, the cash cow resists the use of its cash reserves to help "losers". Several centuries of experience have thus left a minefield of old laws, traditions, and ingrained prejudice to undermine any broad standards for what is best. In no field is this truer than the Medical Industry.
Eighty years ago in Houston, the first Blue Cross health insurance company was started for a single group of school teachers to pay for service in a single hospital. That expanded to other subscribers and other hospitals, soon making it more workable for insurance, subscribers, and hospitals to stand at arm's length, allowing for a variety of local combinations. During World War II, combat in the Pacific led shipyards to be built on the West Coast, but westward migration of steelworkers was hampered by lack of local medical facilities for them and their families. Taking advantage of the loophole provided in the wartime wage and price controls, Kaiser Industries attracted medical personnel by building hospitals, paying salaries, and offering physicians ready-made medical practices. Because of various licensing laws, Kaiser's medical enterprise was divided into two corporations, Kaiser and Permanente, so a specialized corporation within the Kaiser-Permanente Foundation could accommodate the licensed practitioners. The salaried nature of the physician organization immediately caused trouble with local fee-for-service practitioners, who were thus excluded from a large population in their neighborhood when they could not readily adjust to varying mixtures of the two payment methods. Their reaction, led by an obstetrician in Stockton, California, was also to organize dual-corporation structures which were exclusively fee-for-service. Because Kaiser had a Foundation, they also called their organizations Foundations for Medical Care. Then, as now, it proved difficult to run a practice with two different reimbursement philosophies in the same waiting room; in time, friction between the two styles tended to increase as doctors who were more comfortable with each style tended to segregate themselves. Since offers of salaries are more immediately attractive to newly-trained physicians, they flocked to California to serve the steelworkers who were in need of doctors. Fee for service, on the other hand, allowed the gradual assembly of a more durable practice composed of patients who could test what they liked before making a permanent allegiance. Essentially, the transients went to Kaiser, more permanent settlers used fee-for-service.
Thus, it came about that several models for health care reform were tested in a few smallish towns of central California. These demonstration experiments may perhaps not meet everyone's standard for scientific purity, but at least they were public examples with the dumber features knocked away. They certainly provided a laboratory where ideas could develop about topics that otherwise were merely opinions and unsupported conjecture. The Foundations demonstrated that physician-dominated organizations could contain costs and maintain quality in a satisfactory way; there had previously been doubted about their ability to contain cost. The Kaiser organization showed that salaried practice performed acceptably as well, both to most staff physicians and to a majority of the patients; there had been doubt about the willingness of the public to limit choices to a panel of assigned physicians, mostly young and usually from elsewhere. Finally, the two systems seemed to be able to live together more or less peacefully; indeed, the California public seemed reassured that two systems apparently kept each other in check.
The first main difference rested on the system of quality control. The local Foundations developed review systems based on peer review and peer pressure; these worked remarkably well, particularly in constraining non-physician costs like pharmacy, tests, and hospitalizations. Cost and quality control in the Kaiser system was more rule-bound and quicker to apply discipline, kept within bounds however by the ability of both patients and staff to jump ship for the other system. Aside from professional peer review, the Kaiser system experimented with owning hospitals, laboratories, pharmacies. Here, the experience directly paralleled the experience of manufacturing industry with its suppliers; when reimbursement was generous suppliers generated welcome revenue. When reimbursement was constrained and substandard, ancillary service losses were unwelcome. Taken overall, the Houston experience was repeated, that ownership of such facilities was mostly a headache. Indeed, subsequent experience has shown the two systems usually co-exist nicely within independent ancillary facilities.
The Stockton, or Foundation for Medical Care, approach grew popular in the West. The variant which grew up in Utah was locally popular and attracted the attention of Senator Wallace Bennett. The Bennett Amendment to the Medicare Act then picked out the peer review system as the secret of success and set up a nationwide system of Professional Standards Review Organizations (PSRO) to conduct peer review of Medicare and Medicaid patients. The drawing of boundaries around these organizations was the most difficult part, and sometimes the boundaries were inept. Rural districts were adamant that the standards of big-city medical schools were not to be applied to their scattered resources, and urban areas saw themselves as ancient Rome surrounded by hostile tribes. Although these difficulties were foreseen, it is not always possible to draw a line that will separate the cultures, particularly where the outward migration of suburban housing was more rapid than the construction of suburban medical facilities, leaving the medical culture unstable. The PSRO system was quite successful in many areas but caused trouble in others that were not adequately addressed. The central concept of the review system was that the doctors who worked together could quite readily identify the outliers, and better than anyone else could judge whether the local situation was justified. True, some practitioner might try to abuse the system to the disadvantage of his competitor, so no adverse decision was final until there had been an opportunity for outside appeal. There might even be a few circumstances requiring a still higher appeal. The system was new and untried, but it produced eminently satisfactory results from the point of view of the Federal Government paying the bills. As former President of one of the largest PSROs in the country, I will assert that there was remarkably little friction or resistance in the medical community. My very good friend, the President of the New York City PSRO says much the same, and most people would say that if you can carry off a new system in New York without a lot of argument, it must work pretty smoothly. The Government wanted to eliminate unnecessary Medicare costs, particularly in hospitals, and it wanted to maintain peace with the medical profession. Hospital costs are obscured by the wide gap between posted charges and true underlying costs, compounded by disagreement about the proper assignment of overhead charges. Charges were not the assignment of the PSRO, utilization was. Days of hospitalization per thousand enrollees fell from roughly 1000 days per thousand to roughly 200 days per thousand, and that satisfies me at least that we were doing our job; physician peer review was doable.
It is likely, however, that peer review was much more apt to produce friction in rural districts. Philadelphia has had more than a hundred hospitals for more than a century. Birds of a feather tend to flock, so the sorting-out process was already far advanced by the application of constrained referrals to practitioners who failed local standards. Mixing members of different hospital staffs on appeals committees was easy in the big cities, and the naturally censorious tendencies of many physicians could be safely counted on to produce adversary balance. Most committees seemed visibly pleased, even relieved, to discover generally good quality in their competitors' practices. However, in the much smaller and more scattered institutions in the nation's regions with low population density, these informal arrangements cannot stretch as well. When there is only one specialist in a field, for example, it is sometimes hard to know whether he is a good one or not, but always easy to say whether you like him or not. Where the population thins out, much greater wisdom is required to make judgments, the number of close cases is greater, and the limited supply of judicious reviewers is similarly stretched. At least that is my surmise, based on knowing the background of most of the AMA delegates who eventually voted 105-96 to condemn the program in a standing vote. The result was the Dornenberger Amendment, which much weakened the system when instead it should have triggered a more profound analysis and reconsideration.
Perhaps we spend too much time here describing a technical process. It is, however, at the heart of what makes the Foundation approach (sometimes called IPA or Independent Practice Association) superior to the HMO. It is now perfectly clear that both doctors and patients vastly prefer the IPA approach to the HMO, and any reasonable politician would jump at it. But there is one fear, summarized by the slogan that the Fox is guarding the Henhouse. In both systems, an attempt is made to combine insurance with the delivery of health care. In the IPA, the physicians are taking the financial risk that aggregate income will exceed aggregate costs; it's a risk contract. In the case of an HMO, the employer or the government is taking the financial risk and therefore wants to control it. If revenue is good, the doctors will prosper in an IPA; the insurance company intermediary will prosper in an HMO. Doctors will care about that little difference, but why should the rest of the country care?
Because the prospect is overwhelmingly likely that future revenues will be constricted until something hurts, and when you starve with a tiger, the tiger starves last. In the case of an HMO, the insurance middlemen will starve last, and the quality of health care will starve fairly early. That's an unwise design. When we get to the point where Congress cuts the budget and watches to see what happens, Congress will cut it some more if nothing bad happens; it will back off only if something bad happens, so something bad is certain to happen. In designing the system, you need to design the internal review authority so it will cut the waste, inefficiency, and luxury first. The reviewer, no matter who it is, will cut himself last, so you need to arrange the incentives for waste to be cut before the reviewer suffers, and quality of care only after the reviewer has suffered. If you wonder why a whole lot of special interests hate physician-dominated review systems, a short answer will be found in this synopsis. A special exception must be devised for rural health systems, which do have a unique problem.
To return to the well-worn slogan about foxes and henhouses, we have overlooked the central question. Who's the fox, and who is the hen?
The American Health Non-system

|
| Dr. Jock Murray |
Dr. Jock Murray has recently been Chairman of the American College of Physicians. He is also a Canadian. Recently, he was invited to address the College of Physicians of Philadelphia on an evaluation of the lessons to be learned from comparing the health systems of the two neighboring nations. It was an excellent, fair, and well-balanced address. The man who introduced him referred jokingly to the American non-system and Dr. Murray emphasized two epigrams about national systems in general. No nation on earth can afford to fill all of the health demands of all its people. So, all nations confront the three main demands, to deliver everything, to deliver it to everyone, and to do so immediately (ie without waiting lists). Fulfilling any two of these three demands is possible, but to deliver all three is impossible. Comparison of health systems in various countries amounts to identifying which two of the three they have chosen to have, which one they choose to surrender. I hope and believe Dr. Murray would mostly agree to this caricature of his remarks.
As a member of his audience, it does seem to be fair to acknowledge we have a non-system, and probably even fair to go further and observe we fundamentally resist those irksome constraints implicit in having a planned system. No organized system, and proud of it. But we do have something else. Let's call it a vision.
Without formally stating it, or even widely acknowledging it, Americans seem to have embraced a dream that we can indeed have everything for everybody right away. Yes, we can. The method available is to gamble that research can eliminate the disease. We hope, although we know it is not certain, that cancer, schizophrenia and Alzheimer's disease will reduce the cost of care. Our model exists in Rheumatic Fever and poliomyelitis, for which there are essentially no remaining treatment costs. We know that everyone ultimately dies of something; we assume we are already paying everybody's terminal costs. Eliminating diseases postpones terminal costs, but surely does not add to them.
We have knowingly and recklessly embarked on a program of pouring huge amounts of money into medical research. I believe the public mostly suspects that much of our present high cost of health insurance eventually finds its way into supporting research, and the public mostly acquiesces in whatever cost-shifting is involved. The people who devote their lives to research in turn vaguely recognize that we might reach a point where the country cannot afford this gamble any longer, and they could have half-wasted a career. We all vaguely understand it's a gamble; major elimination of disease might not be just over the horizon and might lead us on to indefinite postponement of a foolish dream.
But those are the chances you take; we seem resolved to take them. We are going to give it a go. If we can, we are going to spend whatever it takes to give everything to everybody, right away. We are going to eliminate diseases, on the unproven but plausible assumption that doing so will eventually bring costs down.
Immigration and Universal Health Insurance
Among the many articles about the economic wonder of Dubai,

|
| Immigrants |
along the Persian Gulf, is the comment that only 20% of Dubai's residents are citizens of that country. The other 80% seem to be immigrant workers, flocking there to make $2 an hour because at home they can only make $1. America only has 12 million illegal immigrants at the moment, but comparing our problems with such extreme cases sharpens the discussion.
No matter what position you take on the question of universal American health care or universal anything else for that matter, you eventually have to re-examine your beliefs about our national borders. It is plainly absurd to propose that America should provide health care for the whole world, but if we allow essentially unlimited immigration it comes close to the same thing if you provide health care for everyone who is here.
The reason Dubai is a useful example is that we, too, are working our way into the fix of basing our prosperity on immigration we cannot handle. In recently seeking bids for a new roof, the choices I received were from Costa Ricans, Poles, and Puerto Ricans. True, one American citizen did inquire, but he was merely a contractor for some others, who were almost surely illegal migrant workers. Following the advice of a friend, I chose the Costa Ricans because they were rather small in size; my friend said they were less likely to get hurt falling off the roof. Although the situation in Dubai is more advanced, we seem to share the same difficulty that our economy would become pretty unworkable without immigrant labor. That problem for us does introduce an element of fairness into providing health care for people we really do depend on, or you could adopt the line that issues of practicality urge us to find a solution. Either way, you confront a dilemma, a problem offering two solutions or possibilities, of which neither is acceptable. Perhaps at least we could invent a new term, a multi lemma, defined as a problem with lots of solutions, none of which would work.
Chester: To the Dark Tower

|
| William Penn |
Chester is the original word for Castle in old English, and accounts for towns called Manchester, Lancaster, Dorchester in the Midlands of England. Although much is made of his Welsh ancestry,William Penn grew up and lived in the neighborhood of Manchester. When he first landed in his new colony, he named the place Chester before deciding to move upriver to be above the mudflats and snags at the abrupt turn of the river where we now have an international airport. On several occasions, this protection from pirates and invaders made it possible to remain rich and prosperous without abandoning Quaker pacifist principles. As a further bit of history, the second public reading of the American constitution took place in the courthouse at Chester. During the industrial revolution, Chester became a mighty industrial town somewhat in advance of Philadelphia. The industry has, sadly, abandoned Chester.
Chester repeats the age-old tradition that slums are created when towns are abandoned, making cheap housing available. There's even a particular Chester twist to this principle: the old Sun Shipyards have been turned into a casino. Now, that will create poverty if anything will.

|
| Amtrak's Northeast Corridor |
Peter Barrow is a local real estate man who is determined to lead a revival of the old Chester, and certainly makes a good case for its future. Although much of the city was abandoned, the infrastructure remains. The roads, sewers, water supply, railroads, port facilities may be old but they are essentially intact, making revival much cheaper. Chester is still served by the R2 train from Philadelphia to Wilmington, and is on the main line of Amtak's Northeast Corridor. It's now near the airport, and near the electronics industry developing in Chester County along Route 202. Those things are economic drivers, and they are social ones, too. The old Chester urban Democratic machine and the rural Delaware County Republican machine can no longer afford to remain ossified in perpetual denunciation, in the face of new residents with new outlooks on things. So, there's agitation for reforms and both votes and discontent to propel it forward.
Given a magic wand, the one thing Mr. Barrow would change would be education. The public schools are undisciplined and unsafe, and mobilized by the teachers' unions to resist charter schools no matter what. Things have even gone to the point where Widener University is thinking about starting a charter high school, and the more graduates of charter schools the more momentum builds up for still more charter schools. Hidden in this struggle are two less defensible issues: parochial schools and vocational schools, pro, and con. The struggle over church schools goes back to the founding of our country in the sixteenth century and firmly resists any objectivity about whether parochial schools are better schools, or not. For them, that's not the point. The other tradition at play here is the historic opposition to vocational schools by trade unions. This one might be a little easier to work with since resistance to the development of more plumbers and carpenters was understandable enough during the industrial days of the city, but really is no longer relevant in an era when we now must import illegal immigrants to serve our needs in the mechanical trades.
Chester seems to have a chance to get its act together. Success or failure of this important the struggle could well depend on one or the other of the entrenched political machines, urban and suburban, seeing an opportunity -- and grabbing it.
WWW.Philadelphia-Reflections.com/blog/1322.htm
SCORE

|
| Mark Maguire |
Frank Pace, formerly Secretary of the Army, founded SCORE, the Service Corps of Retired Executives, in 1964. Philadelphia was one of the main founding chapters but tended to dwindle as business large and small dwindled after the bombing of West Philadelphia by the then-Mayor; former executives living in the suburbs lost interest. In December 2006, Mark Maguire took charge and gave SCORE a new direction. This former executive of Rohm and Haas is not related to the baseball home-run king, but at least his name is easy to remember.
The new sociology of center city demanded that more small businesses be started by minority residents, who have very little family and cultural experience in this sort of activity, which nevertheless is recognized as the main source of job creation in any area. It turns out that the main source of energy in the minority community is among minority women, who are particularly unfamiliar with the problems of small business. So, SCORE needs to dispel a number of misconceptions and unrealistic ambitions, and familiarize these budding entrepreneurs with the tax and regulatory headaches ahead of them, and teach them to be watchful of common traps and obstacles, learn to cope with fair competition, and how to recognize the signs of fraud before it happens to them.
The usual vehicle for teaching these elements of commercial life is to induce the writing of a detailed business plan, which executives can criticize for lack of realism or inadequate capitalization, suggesting ways to succeed in a field that experiences 50-60% failure in the best of circumstances. Some of this requires face-to-face discussions, lectures, and required reading. But much of it can be handled with weekly email consultations, a favorite tool of Philadelphia's SCORE chapter. Much of it can be addressed by referring the client to the proper agency or service business, or bank. SCORE has a strict ethical code for its volunteers, including a prohibition of becoming a vendor or participant in the business.
In addition to the changing nature of new small businessmen, there is a changing demographic of the volunteer executives who do the advising. Over 80% of them describe themselves as retired, but in fact, it is rare for one to be totally retired from all business activity. These guys really like to work, and a thirty-year vacation is not their goal in life. Just by acting as an example, they are establishing an important goal for the young businessmen and women who look to them for guidance. Work is how you accomplish something in life, and work, believe it or not -- is fun.
www.Philadelphia-Reflections.com/blog/1430.htm
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
According to the records of the Pennsylvania Hospital, the following 48 persons were patients in the hospital on July 4, 1776:
| Richard Brinkinshire (Admitted 11/15/1775) | John Ridgeway (Admitted 12/26/1775) |
| James Chartier (Admitted 1/6/1776) | patient (Admitted 1/6/1776) |
| patient (Admitted 1/20/1776) | patient (Admitted 1/20/1776) |
| Mary Yell (Admitted 2/7/1776l) | John Beckworth (Admitted 2/7/1776) |
| Bart. McCarty (Admitted 2/10/1776) | John King (Admitted 2/10/1776) |
| Robert Alden (Admitted 2/17/1776) | William Patterson (Admitted 3/6/1776) |
| Elizabeth Hanna (Admitted 3/9/1776) | John McMahon (Admitted 3/13/1776) |
| Mary Burgess (Admitted 3/23/1776) | Mary Anderson (Admitted 4/10/1776) |
| John Hatfield (Admitted 4/15/1776) | Eliza Haighn (Admitted 4/17/1776) |
| Charles Whitford (Admitted 4/24/1776) | patient (Admitted 5/8/1776) |
| Susanna Carrington (Admitted 5/8/1776) | patient (Admitted 5/8/1776) |
| William Johnson (Admitted 5/13/1776) | Lazarus Chesterfield (Admitted 5/22/1776) |
| Mary Spieckel (Admitted 5/22/1776l) | William Edwards (Admitted 5/22/1776) |
| patient (Admitted 5/23/1776, Lunatic) | Jane White (Admitted 5/25/1776) |
| Charles McGillop (Admitted 5/29/1776) | ---Fitzgerald (Admitted 6/1/1776) |
| Michael Rowe (Admitted 6/6/1776) | patient (Admitted 6/6/1776) |
| John Hughes (Admitted 6/12/1776) | Joseph Smith (Admitted 6/15/1776) |
| Esther Munro Lunda (Admitted 6/15/1776) | Mathew Coope (Admitted 6/19/1776) |
| Anne Patterson (Admitted 6/19/1776) | Thomas Savoury (Admitted 6/20/1776) |
| Rebecca Winter (Admitted 6/26/1776) | Elizabeth Manning (Admitted 6/26/1776) |
| Negro (Admitted 6/24/1776) | Elex. Scanvay (Admitted 6/24/1776) |
| Fanny Stewart (Admitted 6/24/1776) | Peter Barber (Admitted 6/29/1776) |
| Catherine Campbell (Admitted 6/29/1776) | Ann McGlauklin (Admitted 7/3/1776) |
| Elizabeth Lindsay (Admitted 7/3/1776) | Ann Jones (Admitted 7/3/1776) |
The records indicate the following diseases were the reason for admission of those patients. Although in Colonial times there was no medical delicacy to avoid offending readers, present privacy standards require that we strip the diagnoses from the name of the patient and list them independently. There is some overlap, sometimes making it difficult to judge which disorder caused the admission.
- Sore, poisoned or ulcerated legs: 16 cases
- Lunacy, mind or head disorders: 10 cases
- Syphilis: 7 cases
- Fever and Rheumatic fever: 7 cases
- Dropsy: 5 cases
- Gunshot: 4 cases
- Diabetes: 1
- Blindness with clear pupil: 1
- Spitting blood: 1 case
- Dislocated arm: 1 case
- Inflammation of face: 1 case
- Scurvy: 1 case
- broken arm: 1 case
The following physicians were elected at the Managers Meeting dated 5/13/1776:
- Dr. Thomas Bond
- Dr. Thomas Cadwalader
- Dr. John Redman
- Dr. William Shippen
- Dr. Adam Kuhn
- Dr. John Morgan
Nation's First Hospital, 1751-2016

|
| Pennsylvania Hospital |
As commonly stated in medical history circles, the history of the Pennsylvania Hospital is the history of American medicine. The beautiful old original building, with additions attached, still stands where it did in 1755, a great credit to Samuel Rhoads the builder and designer of it. The colonial building on Pine Street stopped housing 150 patients around 1980, supposedly at the demand of the Fire Marshall, although its perpetual fire insurance policy still owes the hospital several thousand dollars a year as an unspent premium dividend. There may have been one small fire during two centuries of use, but its true fire hazard would be difficult to assert. It was just out of date. The original patient areas consisted of long open wards, with forty or so beds lined up behind fluted columns, in four sections on two floors. The pharmacy was on the first floor, the lunatics in the basement, and the operating rooms on the third floor under a domed skylight. It was entirely serviceable in 1948 when I arrived as an intern doctor. Individual privacy was limited to what a curtain between the beds would provide, but on the other hand, it was possible for one nurse to stand at the end of the award and recognize any distress among forty patients immediately. In this trade-off between delicacy and utility, the utility was certain to be preferred by the Quaker founders. Visitors were essentially excluded, and if a patient recovered enough to be unnaturally curious about neighboring patients, well, he had probably recovered enough to go home.
Located between two large rivers, South Philadelphia up to ten blocks away was essentially a swamp until the Civil War. So, there were seasonal epidemics of malaria, yellow fever, typhoid, and poliomyelitis at the hospital until the early twentieth century. Philadelphia was a port city, so sailors brought in cases of venereal disease, scurvy, even an occasional case of anthrax or leprosy. During the Industrial Revolution of the nineteenth century, tuberculosis, rheumatic fever, and diphtheria were part of clinical practice. But underlying the ebb and flow of environmental effects, there was a steady population of illness which did not change a great deal from 1776 to 1948. These patients were all poor, because the rules in Benjamin Franklin's handwriting restricted service to the "sick poor, and only if there is room, for those who can pay." In 1948 there was a poor box for those who might feel grateful, but no credit manager or official payment office. The matter had been considered, but the cost of collection was considered greater than the likely revenue. When Mr. Daniel Gill was offered the position as the hospital's first credit manager, it was suggested that he be given a tenth of what he collected. To his lifelong regret, Dan Gill regretted that he refused an offer that he had felt he could not afford to accept.
So, the wards were filled with victims of the diseases of poverty, punctuated by occasional epidemics of whatever was prevalent. And a second constant feature of the patients was their medical condition forced them to be housed in bed. For centuries, physicians dreaded the news that a new patient was being admitted with "dead legs".
Volunteerism Needs a Business Plan

|
| Alexis de Tocqueville |
The visiting Frenchman Alexis de Tocqueville was struck most by the volunteerism he found everywhere in the young American nation; in his view, the first reaction of 19th Century Americans to a problem was to create a volunteer organization to fix it. Benjamin Franklin, who created dozens of such initiatives, was held up as its great exemplar. But de Tocqueville visited us at the beginning of the Industrial Revolution, and we are now well past that into the Information Revolution; volunteerism has noticeably declined. Not only have the great volunteer organizations like the Masons and the Red Cross suffered, but it is far more difficult to enlist the help of others to form a pick-up group to attack some issue or other. It is in that sense the general spirit of volunteerism has declined. The likely difficulty is not selfishness, but the helplessness of people to control their own time.
When volunteer groups to assemble, they are mostly composed of self-employed people like plumbers and dentists, free to be somewhere else during "normal business hours", which although shorter than they once were, seem extended by commuting time and by chores pushed aside during workplace confinement. To some extent longer commuting distances make it physically impossible to do personal chores in the vicinity of the workplace. But constrained personal time is also related to increased control behavior by management. A successful big business has to employ strategies to get employees with cell phones to stick strictly to business while the employer is paying for their time. Now that so many women are going out to work, the family unit needs to struggle to coordinate everyone's work time so there will be some remaining opportunity to conduct family life. When a working couple shares the home tasks and babysitting, the preempted time now extends to two working partners, and what is left is called "quality time". A probably temporary elaboration of this time competition is the need to chauffeur teenagers to their resume-enhancing activities. For the time being, you don't pick a college, the college picks you, and parents desperately labor to assist their children on a career path. Quite obviously, America needs to evolve better ways of trading work at home for more flexibility in the actual workplace, and we also need to build more first-rate colleges, but those issues are not the present topic. To summarize: It's awfully hard to assemble a group of volunteers simultaneously because employers have so successfully assembled their time. Failing to appreciate the tradeoffs inherent in commuting time is a secondary but still important factor, somehow related to the recent housing/schools mania.
Consequently, volunteer organizations increasingly tend to regard their chores as something you hire someone else to do if it proves impossible to dump them on someone who is retired or unemployed, or too timid to refuse. Even nominal volunteers are reluctant to step forward. This leads to recruitment lectures along the line that naturally you must sacrifice if you really truly believe in the goals of the dear old Whatsis Association, surely just a coercive speech pattern. That claptrap was never heard during the age of universal volunteers; volunteering was just one of those things everyone expected to do to get community activities accomplished. We're losing something important if we continue to endorse this attitude. Sometime during the first twenty-four hours in military service, for example, someone will surely advise the new recruit -- never volunteer.
For a penniless non-profit to adopt the solution of hiring staff when there is no revenue stream to pay them, is the first step toward the dissolution of the organization. Essentially, the non-volunteers are ordered to contribute money if they choose to be draft-evaders, and eventually, the officers and staff begin to look back at the organization members as cows to be milked. A class of people who are only making a living is substituted for those who understand and promote the goals, and it just goes downhill from there.
Instead, all volunteers really must each do some unpaid work, and the officers and directors must set an example of it. What an organization does next is crucial. Individual members, either anonymous or hoping to remain anonymous, must be approached with the suggestion they accept responsibility for a task. The wild-eyed response to this approach is quite familiar, like the lame excuse that there is no time. A counter response that I'm busier than you are, does not improve the conversation because it suggests the refuser is merely a selfish shirker. Instead, initial requests must take the following form: They should be for a simple, limited task without any obligations stretching to infinity. Almost everyone will be glad to bake a cake for a party, but almost no one will agree to be chairman of the cake-baking department unless the boundaries of that commitment are more reliably limited than they usually are.
In modern times, any major undefined volunteer responsibility is seen as potentially leading to an unthinkable conflict with gainful employment or else its ill-considered outgrowths like commuting. Since that's the basic problem, all-volunteer invitations must respect the true issue and devise workable ways to circumvent it. Role models certainly help if you have any.
www.Philadelphia-Reflections.com/blog/1448.htm
Urban Bridges

|
| Reverend Mary E. Laney |
The Reverend Mary E. Laney recently told the Right Angle Club about her experiences in an Episcopal mission church, along with the history behind this innovation, and the establishment of a 501(c)(3) organization to help the idea on a national level. That may mean no more to readers of this site than at first it probably did to the Right Angle Club, before Mary Laney made it all come alive. It was quite moving.
|
| Bishop Alan Bartlett |
During the 1980's she asked Bishop Alan Bartlett, at that time the Bishop of Eastern Pennsylvania for the Episcopal Church, if she might be assigned to an urban mission. As ethnic and religious population migrated around the Philadelphia landscape, quite a few Episcopal churches have been stranded in economically depressed neighborhoods, unable to afford a full-time pastor. The concept of a mission church was developed as a designation for churches that had dwindled to the point where only a handful of parishioners were left and were assigned to a category in which the Bishop would appoint a part-time Vicar to be in charge of what then needed financial support from the main church. Although in a sense Bishop White started the idea two hundred years earlier, there were no mission churches in Philadelphia in colonial times, but there are now over fifty of them, a quarter of the Episcopal churches in the region. Reverend Lancey was assigned to St. Gabriel's at the corner of Front Street and Roosevelt Boulevard, and stayed there fifteen years. She is now with St. Christopher's in Gladwynne.
The initial concept was to identify eight lead mission churches, build them up to be self-sustaining, and then replace them with eight new ones. With all good will and hard work in the world, this concept failed, largely because the social conditions of the poor at that time also depressed their educational level, and had instilled in them a culture of constant failure. In one telling episode, the parishioners said there was no hot water in the church. As a matter of fact, the pilot light of the hot water heater had gone out, and the parish was so sunken in the mindset of failure and despair they had not even looked into it. Mary Laney decided something had to be done to change the model.
What seems to have worked was the creation of a 501(c)(3) organization called Urban Bridges. The original idea behind this organization was that since the Constitutional separation of church and state precluded government grants to church no matter how struggling, but perhaps a tax exemption would make it possible for private donations to accomplish what was needed. There was, in addition, the sad experience that whenever the constitution barriers had somehow been overcome by circumvention, the many layers of bureaucracy usually consumed the money. It had proved disheartening to see four or five years go by after a government grant, with not a cent getting to the programs and all consumed by consultants, advisers and supervisors.
Meanwhile, the poor parishioners continued to base their hopes on this sort of relief, while neglecting things which might be more effective.
The Urban Bridges program evolved from a primarily fund-raising organization into a system of partnerships between prosperous suburban churches and the struggling urban missions. The suburban churches proved to be inspired with a wish to help but frustrated by a lack of means to do anything effective. It thus evolved that the suburban Episcopal churches supplied what was really most needed: practical examples of leadership on a local level, combined with visible evidence of successful effort. Literacy courses, drum and bugle instruction, computer tutoring and a variety of other spontaneous activities led to the example of leadership, and in the long run, was a far more effective fund-raising tool than printed appeals and button-holing. Even in the case of crime, it was the leadership that made the difference.

|
| St. Christopher's Church |
The story was told of a drug dealer in the neighborhood who dominated the streets with dogs and blocked access to schools unless the children agreed to sell drugs for him. Local police had proved unhelpful, and hopelessness was rampant. What would prosperous suburbanites do in such a situation? Obviously, suburbanites would not stand for such a situation and called in the Federal Drug Enforcement Agency. The crook was promptly deprived of his dogs and now resides in jail. That may not be wholly in the spirit of peaceful reasoning, but it's the American Way, all right. This was what seemed to be missing in the culture of poverty. It's the determination that whatever the cost, intolerable things will not be tolerated, combined with absolute faith that the system does provide ways to be effective without becoming either lawless or wards of the state. This is America, right?
Edgar Allan Poe, 1809-1849
|
| Edger Allan Poe |
Between the Federalist period and the Civil War, Philadelphia quadrupled in population, mostly by Irish and black immigration responding to the urbanization induced by the Industrial Revolution. The social boundaries of this period were established by the U.S. Capital moving away to Washington, and at the other boundary, the constrained urban population was suddenly released to the suburbs by the City-County Consolidation of 1854. During that time, the Northern Liberties on the other side of Callowhillwere very close by, but nearly devoid of law and order. At least along the Delaware River, the scene was like Las Vegas as imagined by Charles Dickens. Within the increasingly congested boundaries of the city itself, tuberculosis, alcoholism, riots and religious revivalism are all mentioned prominently. While it was the time of Nicholas Biddle and the Bank, and the establishment of the Drexel empire, it was a gothic period quite adequately symbolized by Ethan Allan Poe, writing for Graham's Magazine. His father abandoned the family, his mother and later his wife died of tuberculosis, he was definitely an alcoholic and probably manic-depressive. He and Charles Brockton Brown invented the gothic novel, gothic poetry, the modern murder mystery. Poe only lived in Philadelphia for six years but lived in seven different locations, the most famous of which is now part of the National Park Service, even though it is located off Spring Garden Street. Yes, he was born in Boston but lived there only briefly, and yes, he died in Baltimore, by dropping dead in the street while traveling through. He was scarcely a prototypical Philadelphian, but he was certainly a symbol of his age.

|
| Grip the Raven |
There is a big stuffed Raven named Grip in the Free Library which belonged to Charles Dickens and is claimed to be the inspiration for Poe's Raven; it certainly has an ominous look, whatever its provenance. Poe offered his famous poem to Graham, who rejected it but gave him $15 as an act of charity. Another magazine paid him $9 to publish it. This poem was widely included in elementary school anthologies by the Philadelphia book publishing industry, and its simple repetitions with a scary atmosphere continue to be popular with children. The Murders in the Rue Morgue were the beginning of the modern murder mystery, and seem to have started Brockton Brown off on his establishment of the Philadelphia Gothic novel, echoing the whole dark and menacing Poe tradition. From the descriptions, Poe's alcohol problem was not so much related to the volume of consumption as to the violent manias which just a small quantity provoked in him. If your mother and your wife both died of tuberculosis, it's a fair bet you had it, too. At the age of 40, he was gone.
School Tax Seldom Equates to School Spending
 |
| Little Red Schoolhouse |
As this blog went to press, voters throughout South Jersey had just gone to the polls to vote for school boards and school budgets. Or, at least they had the opportunity to do so, but mostly 15% of eligible voters actually troubled to vote. Meanwhile, school officials chewed their nails in apprehension that many budgets would be disapproved by the taxpayers, and then what? As it turned out, Haddonfield and Moorestown approved their budgets, but over half of the 700 school districts of the state did not. The voters wanted to send a message they were angry about property taxes, and the seemingly related fact that over half of school employees are not teachers. Some of them mistakenly believe county taxes have something to do with schools. If they had really understood the situation, they would have been angry that the size of their local school budget has comparatively little to do with the level of their total tax burden.
Meanwhile, voters with children had been agitating to support the budget or even raise it, even if it raised their taxes; but empty nesters were urging each other to go vote down this budget because their taxes were already excessive. The parents of schoolchildren urged the empty nesters to move somewhere else where they couldn't vote down school budgets. Actually, however, if more empty nesters moved in, property taxes would go down without affecting the school budget, because empty-nesters pay taxes without using the schools. Both groups are quite misguided, however, because raising or lowering school budgets would probably have very little effect on overall taxes. Even school officials failed to make their best case to the public because they misunderstood the tricky way taxes are arranged. They defend every budget by saying it is already cut to the bone. Since it presently makes relatively little difference to overall taxes whether the budget is cut or increased, that's not useful in persuading empty nesters. Budget cutting does make a lot of difference to the quality of education, however, but that's only half of the facts, not a balanced one. The moral of all this is that the voters better get educated about the Jersey political scene, before their children lose the chance to get educated at all.
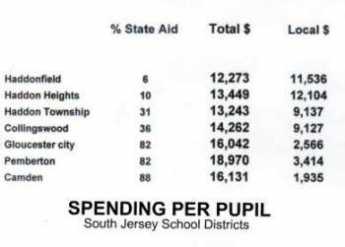
Since I'm an empty nester, I am pretty familiar with the empty-nest viewpoint. Three of my friends have told me they moved to neighboring suburbs in order to lower their tax burden; they undoubtedly know what they are talking about. But no one I know is able to reconcile that fact with the equally certain fact that Haddonfield has the lowest spending on education, per pupil, in the southern half of the state. In fact, they don't care, because they know that local school taxes are significantly lower almost everywhere else, and they don't have to explain why. School officials should be more concerned with explaining their rank in per-pupil spending compared with other districts, but they are driven to make cuts in service where ever they can in order to produce a leaner budget for the voters. They too, seem oblivious to the fact that voter anger won't be soothed for long by their budget cutting because it won't affect overall taxes. Taxes are what people are mad about, but they must consider all of them, and understand that as one goes down, the other will probably go up. In another article, we discuss how they mysteriously go up even more. A more sophisticated view would be that in addition to concern about eradicating poverty in the long run, residents of New Jersey are increasingly driven by the need to get their children into better quality colleges. They would like to improve secondary education to do so but are hampered by the relative unavailability of high-quality colleges in the state. Some of this has to do with the recent tendency of Princeton and Rutgers to seek a geographical diversity of students. But to be cynical about it, the development officers of those colleges know that major donors are to be found in Texas and California. In New Jersey, the majority of income taxes are paid by 1% of the population, and that !% are fleeing the state to avoid its heavy income and estate taxes, just as fast as they can. This is the group that tends to donate most heavily to college improvements, and New Jersey colleges are suffering from their flight. That argument may well be hard to sell in Newark and Camden, but it has a major indirect effect on business creation and employment in the state as a whole.
To return to basics, New Jersey school spending is governed by the Abbott decision, which happens to have been written by a friend of mine, who is a fine, smart, well-intentioned jurist. So-called Abbott districts were found by the courts to have significantly underfunded schools, to the point where it seemed an important public issue that the wealthier parts of the state must help these underprivileged kids get an adequate education. Whether improving the school system in their districts would reduce the crime rate, or welfare rate, among these children in later life, was not then known, but subsequent experience does not give it much support. Mainly, it wasn't so much trying to reduce public expenditures in the long run that was behind the Abbott decision, as the feeling it was the duty of a prosperous society to give deprived kids an even break, a sort of penance for success. Accordingly, state school tax revenues were rearranged in an effort to make the per-pupil spending for education approximately equal in all districts, and particularly in the most deprived areas, the Abbott Districts. The first clear sign that something unintended was happening is shown in the accompanying table, indicating that spending in the Abbott districts was in fact now about fifty percent greater than in prosperous nearby suburbs. Equality might be all right, but fifty percent greater was probably not acceptable to the taxpaying public. Just how that paradox gets accomplished in Trenton is not yet clear, but the discomfort level about it is heightened by noticing there is generally an inverse relationship between the spending per-pupil and the perceived quality of the educational product. You might compare drop-out rates, crime rates, SAT scores or whatever, but public perception is not likely to overcome data seeming to show that the more you spend, the worse the education. One wag commented that the data also seems to show that the further you get from the Delaware River, the lower the educational spending gets; that relationship is also more or less linear. So, what matters here is opinion, and the prevailing opinion is emphatic that this data is upside down. The Abbott decision that school spending must be equalized but is actually greater accounts for much of this funny data, but in addition there almost has to be some overlooked secondary factor which exaggerates the Abbott effect by as much as 50% beyond equality.
Even the education industry has an incentive to explain at least and possibly to correct, this disparity. Because in politics while you can prove almost anything with statistics, it is quite seductive to imply that this data proves that extra educational spending hurts the quality of education, at least above a certain level. The education industry wouldn't be wise to let that sort of accusation go unanswered, even if it comes as a wisecrack. The real empty-nester accusation, sorry to say, is that "My school taxes are way too high. They not only do me no personal good but are not helping underprivileged children, either." The consequence is empty-nesters are driven out of town and out of state, making taxes higher for everyone else. It could take decades to undo this damage with an angered public, so everybody better get to work explaining and correcting the problem.
How Does New Jersey State Aid Affect School Districts?
The Sunday, April 11, 2010 Philadelphia Inquirer contained an eighteen-page statistical summary of the schools within the eight-county area around Philadelphia. The New Jersey school districts, but not the Pennsylvania ones, report per-pupil spending right next to the proportion contributed by a state government. If you know something about the sociology of New Jersey, you form some conclusions about state school aid which probably apply to all states, while confessing they only provably apply to New Jersey. Let's therefore say, it only provably applies to New Jersey that you spend more on schools if you are spending someone else's money.
In the welter of numbers supplied by this statistical report, it seems useful to focus on the strip of school districts along Haddon Avenue, starting from the place where the retreating British soldiers once ferried from Philadelphia to Camden (in 1778, of course.) Haddon Avenue extends directly East until it strikes King's Highway, where the British then turned North to scuttle toward the safety of their navy at New Brunswick. We are thus talking about the school districts of Camden, Collingswood, Haddon Township, Haddonfield and Cherry Hill, with Haddon Heights and Pemberton thrown in because of special features they illustrate.

|
Pemberton Township in Burlington County spends the largest amount of per-pupil school money in South Jersey, $18,970. It jumps right out at you that 82% of that money is contributed to the school district by the state government. Starting back at the Delaware River, 99% nonwhite Camden gets 88% of its school money from the state and has the second-highest spending of $16,131 per pupil. Moving along the path of the British soldiers, the next town after Camden on Haddon Avenue in Collingswood, spending $14,262. Next comes Haddon Township, spending $13,243. It thus seems to prove that the further you get from the Delaware River, the less you spend on education, because next in order comes Haddonfield, with spending of $12,273. But not quite, because Cherry Hill increases a little to $12, 914. The percentage of state funds follows a parallel sequence from Collingswood to Haddonfield (36%, 31%, 6%) and then rises slightly to 11% in Cherry Hill. For comparison, nearby Haddon Heights spends $13,449, of which 10% derives from a state government. And just in case you think there is a racial implication, nearby Gloucester City is 84% white, and gets 82% of the $16,046 it spends on schools, from the rest of the state by way of state contributions. However, these numbers also allow you to calculate how much the local districts spent of their own money. It turns out it is just the reverse. The more state aid a district gets, the less it spends, itself. The more state aid it gets, the more it spends, period.
The conclusion seems to emerge that an education assistance program designed to achieve equality, actually stimulates appreciably more spending in poor districts than in prosperous ones; at least so far, poor educational quality in poor districts is acknowledged to remain poor. There are some people who might say these statistics suggest a racial correlation, but some others could say the correlation is with distance from Philadelphia, while others would associate factors undisplayed in the statistics. Because there are more non-teachers than teachers employed by the schools, it is not certain that extra money going to schools will improve the teaching. Nevertheless, what is not demonstrated at all is a tendency for better education to be found where school money is most liberally applied. At least, it is safe to say that anyone who claims the quality of education parallels these spending patterns in New Jersey, would be laughed at.
|
| Robin Hood |
Of course, it is true that prevailing opinions about the local quality of education are as biased as the opinions about the local football teams, or the differing quality of tomato pies. That's partly because the prevailing opinion of the school system has a strong effect on local real estate values, one of the main concerns of real estate agents. My neighborhood in Haddonfield is very close and sociable, so it's been confided that three empty-nest neighbors have sold their Haddonfield houses and moved to Haddon Heights to save money on taxes. When people make decisions like that, they generally know what they are doing. Available data, however, can be misleading to others because total school spending including subsidies does not reflect local property taxes, while local spending does. Empty-nesters are also very likely downsizing to less expensive homes, where of course the taxes seem lower and are also moving to districts which have fewer children per house. Where that isn't the case in the school districts from which they flee, subsidies are extracted from state income and sales taxes, which move from district to district, right along with empty-nesters who move. For those with children attending public schools, emphasis in these considerations is somewhat different.
The voters have no idea how "equal" became "more" money for education. A fair conjecture would be that the poorer districts kept pressing the legislature for more as a matter of "fairness", leaving the more prosperous districts to shout "outrage", but less effectively. By voting down a majority of local school budgets both groups are shouting, all right, although it would be more effective to shout at their representatives in Trenton. Especially in a census year, when gerrymandering is on every agenda.
Special Education, Special Problems

|
| School Bus |
President John Kennedy's sister was mentally retarded; he is given credit for immense transformation of American attitudes about the topic. Until his presidency, mental retardation was viewed as a shame to be hidden, kept in the closet. Institutions to house them were underfunded and located in far remote corners of a state. Out of mind. And while it goes too far to say there is no shame and no underfunding today, we have gone a long way, with new laws forcing states to treat these citizens with more official respect, and new social attitudes to treat them with more actual respect. We may not have reached perfection, but we have gone as fast as any nation could be reasonably expected to go.
However, any social revolution has unintended consequences; this one has big ones, surfacing unexpectedly in the public school system. For example, the king-hating founding fathers were very resistant to top-down government, so federal powers were strongly limited. So, although John Kennedy can be admired for leadership, the federal government which he controlled only contributes about 6% of the cost of what it has ordered the schools to do, and the rest of the cost is divided roughly equally between state and municipal governments. As the cost steadily grows, special education has become a poster child for "unfunded mandates", increasingly annoying to the governments who did not participate in the original decision. We seem to be waking up to this dilemma just at a time when the federal government is encountering strong resistance to further spending of any sort. The states and municipal governments have always been forced to live within their annual budgets, unable to print money, hence unable to borrow without limit. As Robert Rubin said to Bill Clinton when he proposed some massive spending, "The bond market won't let you."
The cost of bringing mentally handicapped individuals back into the community is steadily growing, in the face of a dawning recognition that we are talking about 8% of the population. Take a random twelve school children, and one of them will be mentally handicapped to the point where future employability is in question; that's what 8% means. Since they are handicapped, they consume 13% of the average school budget and growing. The degree of impairment varies, with the worst cases really representing medical problems rather than educational ones. Small wonder there is friction between the Departments of Education and the Medicaid Programs, multiplying by two the frictions between federal, state and municipal governments into six little civil wars, times fifty. An occasional case is so severe that its extreme costs are able to upset a small school budget entirely by itself, tending to convert the poor subject into a political hot potato, regularly described by everybody as someone else's responsibility. There are 9 million of these individuals in public schools, 90,000 in private schools. They consume as much as 20% of some public school district budgets.
All taxes, especially new ones, are bitterly resisted in a recession. Unfortunately, the school budgets are put under pressure everywhere by a growing recognition that our economic survival in a globalized economy depends on getting nearly everybody into college. Nearly everybody wants more education money to be devoted to the college-bound children at a time when there is less of it; devoting 13% of that strained budget to children with limited prospects of even supporting themselves, comes as a shock. Recognizing these facts, the parents of such handicapped children redouble their frenzy to do for them what they can, while the parents are still alive to do it. It's a tough situation because a simultaneous focus on specialized treatment for both the gifted and the handicapped is irreconcilably in conflict with the goal of integrating the two into a diverse and harmonious school community, with equal justice to all.
As school budgets thus get increasingly close scrutiny by anxious taxpayers, handicapped children come under pressure from a different direction. It seems to be a national fact that slightly more than half of the employees of almost any school system are non-teaching staff. Without any further detail, most parents anxious about college preparation are tempted to conclude that teaching is the only thing schools are meant to do. And a few parents who are trained in management will voice the adage that "when you cut, the first place to cut is ADMIN." Since educating mentally handicapped children requires more staff who are not exactly academic teachers, this is one place the two competing parent aspirations come to the surface.
Unfortunately, the larger problem is worse than that. When the valedictorian graduates, the hometown municipal government is rid of his costs. But when a handicapped person gets as far in the school system as abilities will permit, there is still a potential of state dependence for the rest of a very long life. The child inevitably outlives the parents, the full costs finally emerge. We have dismantled the state homes for the handicapped, integrating the handicapped into the community. But when the parents are gone, we see how little help the community is really prepared or able, to give.
Ruminations About the Children's Education Fund (3)
The Right Angle Club runs a weekly lottery, giving the profits to the Children's Educational Fund. The CEF awards scholarships by lottery to poor kids in the City schools. That's quite counter-intuitive because ordinarily most scholarships are given to the best students among the financially needy. Or to the neediest among the top applicants. Either way, the best students are selected; this one does it by lottery among poor kids. The director of the project visits the Right Angle Club every year or so, to tell us how things are working out. This is what we learned, this year.
The usual system of giving scholarships to the best students has been criticized as social Darwinism, skimming off the cream of the crop and forcing the teachers of the rest to confront a selected group of problem children. According to this theory, good schools get better results because they start with brighter kids. Carried to the extreme, this view of things leads to maintaining that the kids who can get into Harvard, are exactly the ones who don't need Harvard in the first place. Indeed, several recent teen-age billionaires in the computer software industry, who voluntarily dropped out of Harvard seem to illustrate this contention. Since Benjamin Franklin never went past the second grade in school perhaps he, too, somehow illustrates the uselessness of education for gifted children. Bright kids don't need good schools or some such conclusion. Since dumb ones can't make any use of good schools, perhaps we just need cheaper ones. Or some such convoluted reasoning, leading to preposterous conclusions. Giving scholarships by lottery, therefore, ought to contribute something to educational discussions and this, our favorite lottery, has been around long enough for tentative conclusions.
|
Just what improving schools means in practical terms, does not yet emerge from the experience. Some could say we ought to fire the worst teachers, others could say we ought to raise salary levels to attract better ones. Most people would agree there is some level of mixture between good students and bad ones. At that point, the culture mix becomes harmful rather than overall helpful; whether just one obstreperous bully is enough to disrupt a whole class or something like 25% of well-disciplined ones would be enough to restore order in the classroom, has not been quantitatively tested. What seems indisputable is that the kids and their parents do accurately recognize something desirable to be present in certain schools but not others; their choice is wiser than the non-choice imposed by assigning students to neighborhood schools. Maybe it's better teachers, but that has not been proved.

|
It seems a pity not to learn everything we can from a large, random experiment such as this. No doubt every charity has a struggle just with its main mission, without adding new tasks not originally contemplated. However, it would seem inevitable for the data to show differences in success among types of schools, and among types of students. Combining these two varieties in large enough quantity, ought to show that certain types of schools bring out superior results in certain types of students. Providing the families of students with specific information then ought to result in still greater improvement in the selection of schools by the students. No doubt the student gossip channels already take some informal advantage of such observations. Providing school administrations with such information also ought to provoke conscious improvements in the schools, leading to a virtuous circle. Done clumsily, revised standards for teachers could lead to strikes by the teacher unions. Significant progress cannot be made without the cooperation of the schools, and encouragement of public opinion. After all, one thing we really learned is that offering a wider choice of schools to student applicants leads to better outcomes. What we have yet to learn, is how far you can go with this idea. But for heaven's sake, let's hurry and find out.
Mexican Immigration and NAFTA
|
| George H.W. Bush |
The North American Free Trade Agreement (NAFTA) was signed on December 17, 1992, by President George H. W. Bush for the United States, Prime Minister Brian Mulroney for Canada, and President Carlos Salinas for Mexico. It was intended to eliminate tariffs from the North American continent, with long-run benefits for the three nations who made the agreement. Essentially, it was President Bush's idea, growing out of the long period of public service in which he prepared himself for the Presidency in most of the major components of the American government. After his election, he immediately started to implement the many ideas he had formulated, characteristically worked out in considerable detail, and assigned to government officials he had worked with and knew he could trust. The twin results were that he advanced sophisticated ideas much more quickly than is customary, but then experienced backlash from a public which was accustomed to understanding programs before they assented to them. NAFTA was a prime example of both the advantages and disadvantages of an expedited approach.
Tariffs are a tangled ancient political dispute between nations; George Bush got his two neighbors to sweep them away in a remarkably short time for diplomacy. However, plenty of people benefit from the pork barrel, the unfairness and the economic drag of tariffs, so Bush even got ahead of that opposition, essentially presenting it with a done deal. However, he failed to be re-elected because his fellow Texan Ross Perot campaigned as a third party candidate, thundering about a "giant sucking sound" which was predicted as American businesses would flood into Mexico. Whatever Bill Clinton may think, he won the election as a result of the third-party divisiveness of Ross Perot. And Clinton furthermore got to take credit for NAFTA largely because he claimed the credit. Poppy Bush followed Reagan's strategy of winning by letting others take the credit.

|
| NAFTA |
NAFTA had a lot of minor provisions, but the main feature was to help Mexico with manufactures, compensating for America hurting Mexican agriculture with cheaper United States agricultural imports. The usual suspects howled about the unfairness of such a dastardly deed, but they lost. Helping Mexican manufactures took the tangible form of the "maquiladoras", which were assembly plants from the United States re-located just south of the border, assembling parts made abroad into machinery and other final products, for sale in the United States. The general idea behind this was that Mexican immigration was mostly driven by a hunger for better jobs; give them jobs in Mexico, and they would stay home. That's a whole lot better than an endless border war. Even today, it would be hard to find anyone who would contend that fences, searchlights and police dogs were a superior way to control the borders.
For a while, the maquiladoras were a huge success. But then, China got into the act, paying wages so low that even Mexicans could not live on them. No doubt Ross Perot rejoices that the maquiladoras promptly collapsed, leaving abandoned hulks of factories just across the dried-up Rio Grande. And eventually, we even have tunnels bored under the border and more illegal Mexicans in America than we have people in prison who might take the same jobs. Not the least of the consequences came from the other parts of the same country. Mexico traded an injured agricultural economy for the promise of high-paid manufacturing jobs in maquiladoras. So, masses of impoverished Mexican farmers were made available for illegal immigration, up North.
It is now anybody's guess whether Chinese wages will rise enough, soon enough, to reverse the economics of their destruction of the Mexican economy. The election of a union-dominated Clinton/Obama presidency in the meantime does not bode well for actions which would reverse that result, which now would threaten American-Chinese relations of an entirely different sort. It is true that Chinese wages are relentlessly rising, and that transportation costs now favor assembly-factories closer to the American consumer. But maybe the moment for this approach is passing, or possibly has passed.
REFERENCES
| George H. W. Bush: The American Presidents Series: The 41st President, 1989-1993: Timothy Naftali, ISBN-10: 0805069666 | Amazon |
Adoption
|
| Peter Conn |
Peter Conn, a member of the Franklin Inn of Philadelphia, is recently retired from the University of Pennsylvania. Since he has adoption in his family, he became curious about the matter, found that almost nothing has been written about the history of this topic, and decided to write a book about it himself. At a recent monthly meeting of the club, he described his findings, which are pretty surprising.
In a vague sort of way, everyone's general readings do confirm his findings that adoption was frequent among the American Indians, and also among the ancient Romans. In early 6th century Europe, however, it seems to have died out, only to return as a common experience in the 16th century. The first American law that Dr. Conn could find establishing the rules and legal conditions of adoption was passed in Massachusetts in the 19th century, at roughly the time American states were passing laws forbidding abortion. Whether there is a connection between the two movements or not is speculative. However, it does seem pretty likely that our current perceptions about adoption are surprisingly recent, reflecting a strong likelihood that Roman and Indian traditions have nothing to do with it, but fairly recent history might well have a lot to do with it.
Just a little reflection about all the stories we read, alluding to orphanages, foundlings, wards, primogeniture, romantic love, choices of marriage partners, and the like, quickly confirm a realization that conditions and attitudes about reproduction must have changed a very great deal, and fairly recently. It was not very long ago that children were apparently so numerous they could be treated as expendable. Considering how dangerous childbirth has been until recently, current attitudes about "valuable babies" , motherhood, and even the role of women in society must be evolving quickly without our realizing it, and in directions so recent they may well require further revision. Just whose views are old fashioned and whose views reflect modern insights are both judgments we probably should classify as tentative for at least a few more decades.
For example, the dates of major changes in attitudes about foundlings inevitably generate reflections about the attitudes of the Catholic Church. That ancient organization probably has enough troubles with bedroom issues, without adding this one. But the coincidence of the dates with the rise of the Church in Europe, and the subsequent rise of Protestantism, inevitably generate questions about Church attitudes as the cause, or possibly some sociological changes in society which transform both church and reproductive attitudes at the same time. What were the roles of the Crusades, and the Arab invasion of Europe, or the Ottoman invasion? Or the black plague and the white plague, or the Industrial Revolution? We have to know more about these cataclysmic events in order to have even a small idea of whether they might have influenced each other.

|
| Milton Hershey founded the Hershey Industrial School |
It makes a lot of difference whether a culture needs agrarian workers or not, to understand why "the best interests of the child" should only recently have been established as a legal basis for oversight of contested adoptions. Or why inheritance by adoptive children has only been such a recent phenomenon, endorsed by law. What happened to cause the abandonment of all the orphanages we used to have? Why have we chosen to split the issue between adoption and foster care, and treat the two so different? Where do the Girard College and the Hershey School fit into this transition? Why do the Russians feel they are injuring America by forbidding American adoption of Russian orphans?
And get this: during the 19th century in America, when there was a surplus of women on the East Coast resulting from a massive migration of males to the West, about 250,000 American orphans were packed on various trains and sent West. We are told they stopped at a station and let the local settlers select a few, and then the train continued going West, letting off more and more adoptees until they were all gone. Transcontinental railroads were only built after the Civil War, so this sort of child disposal was not more than a century before the political battles of Roe v Wade. We have a lot to learn, and probably a lot to be humble about. So let's not bury the truth under a mountain of political correctness, but let's not have any witch-hunts, either.
REFERENCES
| Adoption: A Brief Social and Cultural History: Peter Conn: ISBN:ISBN-13: 978-1137332202 | Amazon |
| Posted by: Kurt Constantine | Apr 9, 2017 6:35 AM |
38 Blogs
Tax Credit Time
Here's how a discouraging proportion of indigent tax credits go right into the pockets of predators.
Winter of Our Discontent
Medicaid was intended for indigent hospital and physician reimbursement, but state governments have diverted the funds to nursing homes. State governors are defensive about it.
Old Blockley (P.G.H.)
Every Victorian American city had a big medical almshouse, but Philadelphia had the best. The 1965 Amendments to the Social Security Act (Medicare and Medicaid) destroyed P.G. H. at the behest of local hospitals. They now regret it.
Loaves and Fishes
Philabundance comes close to automating the feeding of homeless people, drawing on the techniques of the supermarket chains.
Slum Creation and Urban Sprawl
Suburban sprawl leads to urban home abandonment. Nobody likes the process, but varying factors continue to promote it.
Police Athletic League
The Police Athletic League wasn't invented in Philadelphia, but it has done the city a lot of good.
Settlement Music School
Without much notice, fifteen thousand music students attend six branches of a school with connections to the NAACP, ACLU, and the Bull Moose Party.
James A. Michener (1907-1997)
< James A. Michener was a birthright Quaker from Doylestown, Pennsylvania, where he made his home when he wasn't traveling. He wrote 40 books, most notably "South Pacific", but lived a fairly simple smalltown life, meanwhile giving over $100 million to charity.
Stephen Girard and Religion
The great philanthropist was, to say the least, anti-clerical. A real-life story tells how far this was carried.
The First and Oldest Hospital in America
The history of American medicine is the history of the Pennsylvania Hospital.
Keeping Lunaticks Off the Streets
AFSC: American Friends Service Committee
 Quakers serve, without fear or favor.
Quakers serve, without fear or favor.
Block Captains
A remarkable group of volunteers look out for their neighbors.
Charitable Immunity: An Underestimated Revolution
This particular judge-made change in the laws opened the floodgates for malpractice lawsuits..
House that Love Built: Ronald McDonald of Philadelphia
The idea of a temporary residence for patients and their families near a children's hospital came from Dr. Audrey Evans of Philadelphia. Initial fundraising was driven by Fred Hill of the Philadelphia Eagles. In 25 years, over three hundred others in 26 nations have independently taken up the idea.
Slavery: If This be done well, What is done evil?
 Philadelphia German Quakers were the first to protest the evils of slavery.
Philadelphia German Quakers were the first to protest the evils of slavery.
Insuring the Uninsured is Not Entirely a Health Issue
The health industry resents its unwelcome role as a political tool in the tensions between labor shortages on the one hand, and unemployment on the other.
Unequal Health in an Unequal World
Poor people get sick and die oftener and sooner. But is that because they are poor?
Community Volunteers in Medicine
A little group of medical volunteers in Pennsylvania's Chester County may not understand the underlying issues very well, but they just pitch in and do what they can about the medically underserved.
No Laborer Left Behind
Expanding prestige universities to fill American academic demands, unexpectedly provoke inflation obscured by illegal immigration.
Pennsylvania Prison Society
When the British monarchy put William Penn in jail, they set in motion a social movement which has changed prison management more than it changed Penn.
Picking Up the Usual Suspects
When the U.S. President plans to change health care, everyone involved in healthcare gets excited. Some want to resist change, some want to exploit it, but everyone wants to have influence.
Health Maintenance Organizations (HMO)
Paul Ellwood gets credit for inventing the term HMO, and for selling a version of it to large employers, as well as the Clinton Administration. It's been a bumpy ride.
The American Health Non-system
America is betting heavily that elimination of disease will ultimately reduce healthcare costs.
Immigration and Universal Health Insurance
How can we give health insurance to illegal immigrants?
Chester: To the Dark Tower
 The ancient town of Chester struggles to revive..
The ancient town of Chester struggles to revive..
SCORE
 The Service Corps of Retired Executives has taken a new turn in Philadelphia, primarily serving minority start-ups, a majority of which are founded by black women.
The Service Corps of Retired Executives has taken a new turn in Philadelphia, primarily serving minority start-ups, a majority of which are founded by black women.
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
Patients in Pennsylvania Hospital on Independence Day, 1776.
Nation's First Hospital, 1751-2016
The nation's oldest hospital changed more from 1948 to 2016 than it did from July 4. 1776 to 1948.
Volunteerism Needs a Business Plan
 Volunteerism has declined in recent years because of conflicting demands made by gainful employment. The spirit of volunteerism has not diminished, it just needs a different business plan.
Volunteerism has declined in recent years because of conflicting demands made by gainful employment. The spirit of volunteerism has not diminished, it just needs a different business plan.
Urban Bridges
The Episcopal Church has found a practical way for its prosperous suburban branches to form partnerships with struggling urban parishes.
Edgar Allan Poe, 1809-1849
Edgar Allan Poe may not have the highest literary esteem of any American, but he is probably our most famous poet. At the 200th anniversary of his birth, his disordered life symbolizes an era.
School Tax Seldom Equates to School Spending
Voting today on school budgets, local districts in New Jersey do not seem to realize how poorly school spending correlates with school tax rates.
How Does New Jersey State Aid Affect School Districts?
State aid for schools is like health insurance: costs go up faster when you aren't spending your own money. At least, that's what the New Jersey statistics seem to show.
Special Education, Special Problems
Until recently, mentally retarded children weren't even considered in school budgets. But in recent decades, they have become one of the biggest challenges.
Ruminations About the Children's Education Fund (3)
By selecting children for scholarships by lottery, it emerges that different schools make big differences.
Mexican Immigration and NAFTA
NAFTA was a brilliant innovation by Poppy Bush, but it was perhaps a little too sophisticated.
Adoption
 Although the Romans frequently adopted children, the practice died out in the 6th century, and only became common a thousand years later. Curiously little has been written about this matter, so speculation is probably unwise.
Although the Romans frequently adopted children, the practice died out in the 6th century, and only became common a thousand years later. Curiously little has been written about this matter, so speculation is probably unwise.