2 Volumes
Reminiscences, In Memoriam, The Right Angle Club,
Philadelphia doesn't toot its own horn very much. A central part of its charm is the wealth of anecdotes, and many charming characters, known only to insiders. You have to be a real Philadelphian to know very much of this lore.
Philadelphia Reminiscences
Volume of Philadelphia Historical Episodes
Personal Reminiscences
One of the features of aging past ninety is accumulating many stories to tell. Perhaps fewer are left alive to challenge insignificant details.
My Years at Stockley
For forty-six years, I drove three hundred round- trip miles from Philadelphia to Stockley, Delaware -- once a month on Saturdays. That takes a whole day, so it kind of means I spent a year at sixty miles an hour, going and coming. In Delaware, they speak of going “South of the Canalâ€, to indicate the little state of Delaware is actually two states or at least two cultures. North of the Delaware-Chesapeake ship canal is the posh little city of Wilmington, where most of the major New York banks are moving to enjoy the special banking laws, and where the Dupont family held majestic court over its Ivy League Camelot. Wilmington has more lawyers than anywhere or at least more white shoe patrician lawyers than anywhere. Little Delaware generated special laws for the benefit of corporations, so a whole hive of corporation lawyers generated an industry of pretending that General Motors and IBM are headquartered there. Those lawyers were once so remote from the graduates of second-rate (i.e. state rather than national) law schools making a living as plaintiff lawyers, that even the doctors in Wilmington were on cordial terms with the Wilmington lawyers.
South of the Canal was something else. I saw burning crosses on several occasions, and my trip took me past two race tracks for horses and two for beat-up jalopies that smash into each other for the fun of it. To be fair about it, I was shot at twice, once below the canal, and once in Wilmington, that's another story. The incident below the canal was not terribly spectacular; I just heard a loud noise as I drove past Elks lodge, or maybe a Moose lodge, and there was a nice round hole in my fender when I got out of the car. I suppose someone in the lodge was just careless with his gun, but it is not impossible that I had crowded a pick-up truck which retaliated with fair warning.
I met a nice lady from Rehoboth who tells me she remembers when the highway was built; before 1930 or so, there was no road connecting lower Delaware with the outside world. The native people speak with an accent which isn't quite Southern and which is said to be very close to true Elizabethan English. The area was settled by Swedes before the English came, so the people are quite handsome in a sort of Daisy Mae, L’il Abner way. The highway has an interesting history. Coleman DuPont purchased the land and built the highway at his own expense. If you know anything about rural legislatures, you can guess what happened next. He offered the highway to the State and the legislature refused to accept the maintenance costs. When he then hired his own police force to patrol the highway, the legislature reconsidered and accepted his offer to give them the highway.
My trips to this area have their destination at the Hospital for the Mentally Retarded in Stockley, Delaware. In spite of the way it is spelled, it is pronounced "Stokely". A state cop once forgave my speeding violation when I told him I had been at "Stokely". He said that in spite of my out-of-state license plates, I must be telling the truth if I knew how to pronounce it. The hospital has always kept a sign-in log in the administration building, and it is fun to see my signatures going back to 1958, month after month. I've had a couple of close calls or near-accidents on the highway which I haven't told my wife about, and on two occasions the ice or fog was so bad I had to turn around and come home without completing the trip. The trip ordinarily isn't so bad. The car is on cruise control, there are medical education tapes to play (Audio Digest, courtesy of the California Medical Association), and a sort of hypnosis makes you forget where you are going until you get there.
The medical director is a nice young fellow who has a practice in a nearby (25 miles) town and stops by for a few hours a day. Except for him, just about every resident doctor in thirty years has been foreign-born, and I would judge, very poorly paid. So, several years before I came to Stockley, someone had the idea of bringing in consultants from Wilmington, Philadelphia, and Baltimore. In the early days that was reasonably easy to do, because the hospital was filled with six hundred perfectly fascinating cases. I've seen several albinos and one thirty-year-old who was no bigger than an infant in arms. They used to have a number of cases of grotesque hydrocephalus, where the poor child grew a head larger than you could put your arms around and which would develop huge bedsores because the child couldn't move his head, let alone lift it. Because the Delmarva Peninsula has been a closed society for over three hundred years, there are lots of cases of rare inherited diseases. I have seen many cases of disorders that other doctors have only maybe read about, and I must admit I loved the experience.
But you know after you spend as much time with them as I have, they stop being interesting cases and become individuals, with names and personalities. Since the aging process is accelerated in several common diseases like Mongolism, I have known some of the patients' as little children, then as adults, and finally as dying withered victims of senility. Many times, I have watched the central agony of mental retardation; the children inevitably outlive their parents and ultimately have no one to love them except the institution.
In that role, Stockley does pretty well, although perhaps not as well as it used to do. The switch seems to have happened with the John Kennedy administration when money for the retarded became abundant. That landmark was especially memorable on a Saturday when the Russians menaced us over Cuba. I never knew we had so many eight-engined bombers as circled over the Dover Air Force Base that day. Years later, a pilot brought his son to see me, and I asked him. "Yup," he said. "we were carrying eggs, all right." "Picked them up in Alaska."Ethnic Cemeteries
|
| Ed Snyder |
Schneider spelled Snyder (or Snider) is almost certainly a Pennsylvania Dutch surname in some sense. I presume Ed Snyder is of that derivation, but at any rate, he addressed the Right Angle Club recently on the subject of photographing cemeteries. Along the way, he seems to have picked up a lot of historical facts about graveyards, which he put together into a fascinating story. I get the impression many of the traditions he described originated in Europe and were transported here by various waves of immigration. So we don't have much information about the origins of those customs, except by inference.

|
| Meeting House on 4th |
The Quakers who settled Philadelphia in the early 1680s didn't believe in putting your name (or your picture) on anything, feeling that would be idolatry. The tradition, plus the yellow fever epidemics, accounts for the Meeting House at Fourth and Arch having forty thousand people buried in its yard, in five layers, but above them only two tombstones. Just why those two were exceptions is not described. Jonathan E. Rhoads, the famous University of Penn surgeon, has his name on a pavilion at the hospital to which he raised a loud objection, but he finally died there himself, saying, "It didn't look so bad." So we have comparatively few early Quaker monuments still standing in the Quaker City, although it does seem pretty certain the Quakers are not responsible for the midnight vandalism now sweeping the country, toppling tombstones. In any event, there definitely is an anti-cemetery movement going around our nation, possibly dating back to the days when bodies of parishioners were buried in churchyards if they were in good standing, sort of a giant compost heap. On the other hand, some people remember that Antigone went to some lengths to recover and honor her dead brother on the battlefield of ancient Greece. And that one of the reasons the Romans fed the early Christians to the lions was their horror at the retention of the bones of ancestors in the catacombs. Christians actually took residence in the mortuaries in the expectation of a second coming for everybody. The Mormon infatuation with genetic ancestors may be part of this concept.

|
| Laurel Hill Cemeteries |
It has been said that if you stick a shovel in the ground anywhere, you will encounter a cemetery, but not in Philadelphia. Somewhere around 1830, we imported the French set of traditions of cemeteries, which you can still see as the questionable tombstones of Abelard and Heloise outside Paris. Laurel Hill in Philadelphia was started as an intentional commercial imitation, at a time when you had to take a boat on the Schuylkill to get there, taking the whole family along to have an all-day picnic among your ancestors; and mighty industrial potentate families competed to construct the biggest most expensive mausoleum for the family. Laurel Hill has since fallen into some disrepair, but there is a restoration movement actively repairing it, collecting donations, tracing histories, etc. Neill Bringhurst, a former president of the Right Angle Club, was once the owner, but he vigorously disliked the whole idea and sold it. Woodland, near the University of Pennsylvania, is the other surviving cemetery of this elegance, and it is kept up much better than Laurel Hill, except for the tangled bushes around the periphery to maintain privacy. Woodland is right next to an extensive trolley-car terminal, thus conveying some idea of its former popularity. Prior to being a cemetery, it was the mansion site of Andrew Hamilton, whom George Washington used to visit on his way to Mount Vernon. As you recall, this Hamilton was the original Philadelphia Lawyer, who went to New York to defend the freedom of speech of Peter Zenger the newspaper man accused of telling the truth when he slandered the Governor. Considering the successor governors of New York, it's a good thing he won the case. History has it he was a young unrecognized lawyer, but in fact, Hamilton was the most eminent lawyer of his time, having originally purchased what is now Independence Hall.

|
| Marble Angels |
The traditions of marble angels hovering over tombstones seem to have been imported by Irish and Italian immigrants and are reflected in their present cemeteries. And the Pennsylvania Dutch tombstones and records are intact in Hummelstown PA, dating back to the Seventeenth century. It reflects that this particular branch landed in New York, went up to the Hudson to Kingston, and back down to the Harrisburg area on the Susquehanna. Meanwhile, the Quakers further East were burying their dead in layers without "markers".
There's probably a lot more to this history, but burials are sort of private affairs, so most church groups are unaware of dissenting attitudes, not very far away from them.
The Zimmerman Telegram
|
| Arthur Zimmermann |
Sometime in February 1917, Zimmerman the German foreign minister sent a telegram to the President of Mexico, in code. The Germans sensed their submarine warfare might win the war for them, he wrote, and so it might be very helpful to have a second front attacking the allies' main supplier, the United States. Germany would then win World War I, able to give Mexico --Texas, New Mexico, and Arizona. The British intercepted the telegram, decoded it, and wasted no time putting the translation on Woodrow Wilson's desk.
Wilson had just won a Presidential election on the platform, "He kept us out of the war." Furthermore, the Germans were the single largest ethnic minority in America. But no matter. Nevertheless, within a few days, Wilson stood before a joint meeting of Congress urging them to declare war on Germany.
|
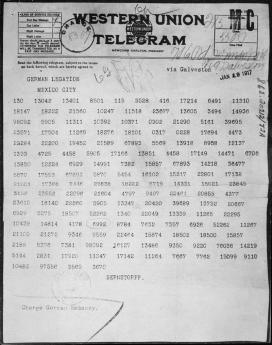
| Telegram in Code |
The consequences were immediate: the German minority was cowed with shame and counting World War II as a continuation of World War I, sixty million people were subsequently killed because of a single heedless telegram. In retrospect, Wilson should have kept it quiet, privately negotiating something from Germany in return for ignoring the thoughtless telegram, and maybe keeping us out of two World wars. That's the sort of thing that gets played around with when a responsible leader creates an uproar over catching an enemy with red hands. Otherwise, the carelessness tempts diplomats to assume he really did want a war, and needed a pretext for it.
It may violate the Constitution or some partisan law created by Congress, but it's the way diplomacy has been conducted ever since--well, since Benjamin Franklin was Ambassador to France, at any rate. It isn't exactly leadership, but it might have saved millions of lives. Muhlenberg told us, "There's a time to preach, and a time to fight." What he seemed to forget was the part about preaching.
Deputy Managing Director
|
| Judge Benjamin Lerner |
The Deputy Managing Director of Philadelphia, former Judge Benjamin Lerner, honored the Right Angle Club by coming to lunch, recently. He immediately improved our opinion of him by first explaining why he resigned as Judge.
It seems the Inside Baseball of the last Mayor's election shifted the politics quite a lot. Under Mayor Nutter, the department heads reported to the Mayor, but under the new Mayor Kenney, everybody reported to the Managing Director. So Judge Lerner promptly resigned his judgeship and became Deputy Managing Director, if you see the drift of the power shift. He had become exercised about the drug problem in Philadelphia, wanted to do something, and knew the ropes to get it done. You've got to like a man like that.
It doesn't matter what happened to get him mad. The drug situation in this town is a disgrace, and any number of reasons might have got the Judge angry. It's too early to know what he can accomplish in his short time in office, but I have every confidence that if he can't improve things, it's time for all of us to move to another city. Because no one can fix it if he can't.
0

|
| Drug Situation |
In fact, I happen to know something he admitted he didn't know. Several years ago I was mugged in the middle of a police stake-out, so they caught the culprit. That's a pretty open and shut case, but the defense attorney apparently tried to stall me out of being a witness. For nine --nine -- consecutive trials, I canceled appointments and appeared at 9 AM. By the afternoon, I sat there waiting to be told the trial was postponed -- for a prisoner in custody, no less. In any event, I then watched nearly a hundred trials during these nine periods, and every one of the defendants told the Judge he had been smoking drugs, outside the courtroom in the corridor. Well, as a witness I was free to walk around, and I can tell you nobody was smoking drugs in the corridor. I knew for a fact they were telling the judge they were addicts when they weren't. I haven't the slightest idea why they were doing this, but I presume they had discovered some loophole in the law and were exploiting it. A rule that drug addicts escape a jury trial might be a plausible explanation, but I simply don't know.
The Judge agreed with me he had no idea of this behavior, or if it continued to happen. But I am willing to bet, it's now going to stop.
Suited To A "T"

|
| Mucous Membrane Pemphigoid |
After sixty years as a doctor, it's a little disconcerting to find I have a disease I never heard of. It's better in a way, but in this sense it is worse, to be cured by a treatment I never heard of, either. The disease is mucous membrane pemphigoid, and the cure is Rituxamide. Am I right? Most readers have never heard of either one, but like just about every other patient, I think you all must just be panting to hear about it.
|
| Rituximab |
It turns out I had heard about the disease, but someone had changed its name from lichen planus to mucous membrane pemphigoid. The drug, Rituximab, has been around since 1997, treating rheumatoid arthritis, so it's not completely novel, either. It simply hadn't been used for this condition, which was rare. When we got semantic issues straightened out, and I had experienced a second round of treatment, I attended a seminar on lung cancer. That's the sort of thing doctors do for entertainment.
To my puzzlement, I was told a "me, too" variant of this same drug extended the life of lung cancer patients, but only if they were heavy smokers who quit smoking. That sounded peculiar, essentially saying you live longer from lung cancer if you smoke heavily and don't quit. You get a little euphoric when you take a steroid drug to ease the Rituximab, so I was overcome with the audacity to go to the microphone and announce I thought they lived longer, not because it helped the lung cancer, but because they lived longer by having fewer heart attacks and strokes from the smoking they had quit. Of course, I was politely told I didn't know what I was talking about. But an immunologist in the audience rose to say he agreed with me, because he had been giving the drug to practically every patient in his immunology practice, and quite a few of them got better. (To explain, the drug knocks out the T cells, which mediate most autoimmune diseases, so it sounded plausible.) So that's where matters stand. After everybody scrambles to try the drug on various autoimmune patients, some sort of order will probably emerge.)
But before everyone who reads this demands that his doctor gives him this drug for itchy skin, let me tell you the subsequent story. My insurance company sent me what is known as an "EOB" (explanation of benefits) which had two numbers on it. In the upper left-hand corner, it said my bill was $67,000. In the lower right -hand corner, it said the amount owed was $0.00. Somewhere between the two numbers is the amount you would have to pay if you didn't have insurance, the rest is someone's mark-up. I set about to find out how much the drug really costs to manufacture, and it's hard to find out. Someone said $4, but I can scarcely believe it.
Litchfield to Wilkes Barre, Today
To go from Connecticut to Pennsylvania without going through New York City seems at first a puzzling proposal. After all, New York is in the way. But a couple of centuries ago the Connecticut Yankees really did make it through the mountains, fought three little wars called the Pennamite Wars, and briefly made Wilkes Barre into part of Litchfield County. Because there has been comparatively little settlement along the trail, taking the trip today is the same mostly mountainous, journey. There are no Indians, but the mountains and rivers are the same. You still have to cross the Hudson, Delaware and Susquehanna Rivers but it's a beautiful trip at any time, particularly so during the autumn leaf season. Litchfield to Wilkes Barre: Millions of people live within a day's drive, but it's a good idea to pack a box lunch and fill your tank before leaving.
Lithuanian Law
The Right Angle Club was recently entertained by its rugby-playing, Kilimajaro-climbing member, John Wetzel, about his two-week stint teaching law students at the University of Vilnius. This ancient Lithuanian institution was founded in the 15th Century by Jesuits, and after a bumpy history of invasions and occupations has now re-established itself. It participates in Erasmus mobility, meaning it is one of 47 European universities which exchange credentials and permit students from any one of them to take courses in any other member of the association; evidently, similar mobility of faculty is also part of the concept. It sounds like a great idea, which American universities might well consider.
For reasons not entirely clear, 75% of the law students at Vilnius are female, and the whole local legal profession is similarly woman-dominated. John made several allusions to the general pulchritude of his students, which a class picture with him confirms. One striking feature of such a picture is how slim the ladies are; this is another European feature our own representatives might consider imitating. Since there are 2500 law students in a country of 3 million inhabitants, whose main industries are agricultural, balance is restored by only admitting 15% of the graduates to a passing grade on the bar examinations. It seems remarkable that studying law remains so popular under the circumstances, but it was explained that most of the graduates end up working for banks or government. Governments including our own frequently feel their laws don't apply to themselves.

|
| University of Vilnius |
If you think about it, a country which is attempting to convert from a Soviet colony to a member state of the European Community has a lot of loose ends to tie up. The title to a property is regularly clouded by the experience of confiscation by the government and then subsequently return to a free economy; if banks accept such collateral, there may well be a lot of legal work to be done to assure its security. Since the thirty-odd members of the European Community all have different legal systems in different languages, all banks and businesses which attempt to operate across borders require partners or consultants in law firms in many countries. While there is a continuous effort being made to establish some uniformity of laws in the various nations of the Community, it takes a fair amount of study just to know what the laws are and how they differ. Therefore, while a handful of lawyers are sufficient to appear in court in disputes and litigation, a great deal more legal background is required, just for businesses to know how they are expected to behave.
Since, as Justice Holmes remarked, the life of the law has not been logic, it has been experienced, it emerges that a great deal of effort must be expended to create the logic when there has been no preceding useful experience. The example is offered of American bankruptcy law, which did not exist until Robert Morris forced its creation. Morris had become an enormously wealthy man, and thus created an enormous tower of debts when his speculations failed, amounting to the then-staggering sum of $12 million of debt. They put him in debtors prison on Walnut Street, but that scarcely addressed the real problems of all those creditors tangled up in the mess. Lithuania is in a similar position, and although it has created a bankruptcy law for corporations, there is as yet no bankruptcy law covering individuals, and hence credit cards, etc. are difficult to establish.
There is a notable difference in attitudes between the eastern nations which were former members of the Soviet Union, and are intensely eager to learn more about the evolution of American law, and the more western parts of Europe, where disdain and hostility for American exceptionalism is presently dominant. A moment of reflection about this difference in a situation should make Americans more tolerant of western European problems. If the logic of law evolves out of the contemplation of experience, it may well be easier to begin without any usable experience, than to begin with centuries of experience which has to be re-examined. It must in fact be a wrenching experience, but one which has the potential to teach Americans a great many things we never had to cope with. The eventual outcome should be a healthy one, providing of course that we can keep our tempers, and acquire a little humility along the path.
Going Down with All Flags Flying
They tell me every man is a little afraid of his father-in-law. I was certainly afraid of mine. He was a giant of a man, and no one called him gentle. As a college student at little Hamilton College, he was named to Walter Camp's All-American football team, subsequent to a famous game at West Point. In those days, wearing a helmet was the mark of a sissy, and kicking the opponent in the groin was nothing much. In off-season, he went out for track and field and held the American record for the forty-pound hammer throw for a number of years afterward. Believe me, he was plenty big. As an intern at the old Roosevelt Hospital in New York, he used to volunteer to ride the ambulance into Hell's Kitchen, mostly for the fun of being able to mix into the bathroom fights.
Now, the really intimidating part of his character as far as a nerdy son-in-law was concerned, was intellectual. His roommate at Hamilton had been Alexander Woollcott, the man who came to dinner. My mother-in-law despised Alexander, as apparently, every hostess did. But my father-in-law enjoyed him thoroughly and would invite him to give a lecture at the local Torch Club in Binghamton as a way of showing the local disbelievers just who really knew whom. My in-laws lived in a small city in upstate New York which seemed to me to have invented the concept of provincialism, but I kept my opinion private. My father-in-law felt no need to conceal his opinions, and that too put me in awe. He didn't go around calling his neighbors a bunch of narrow-minded blockheads, but it was definitely true that his favorite expression was, "Well, that comment of yours is ridiculous, of course." As a man who could hold his own at the Algonquin Round Table as well as against the Army offensive line, he said just about anything he pleased.
I truly believe he was an outstanding physician, although I never saw him in action as a physician. He belonged to some of those snotty surgical societies which would be unlikely to admit a man from a small town unless he had more than distinguished himself. Societies like that do have a certain number of dolts in their membership, but such dolts are almost invariably from Harvard or Johns Hopkins or some similar place where being a sycophant to the society president back at home can occasionally get you admitted as a favor to the great man. That sort of thing is unlikely to get someone admitted from a small town unless he is an individual of unusual distinction. Even beyond such honors, I talked medicine with him quite a bit, and I am left with the feeling that he knew what he was talking about. As we say in the medical locker rooms, he was my kind of doctor.
But one day his time was up. He called us to say goodbye, just before he underwent emergency surgery from which he held scant hope of recovery. His surgeon was much more encouraging to us on the telephone, but when we arrived, he told us of the conversation he had conducted with his patient. As nearly as I can recall what he said, it went like this:
" Dr. Blakely, I think you have appendicitis, and we must operate immediately." "Nonsense. I have mesenteric thrombosis and I Know it."
"No, said the surgeon, "I believe you have appendicitis. It's quite typical."
"Will it do any good to operate on me if I have mesenteric thrombosis?"
"No," replied the surgeon. "But I believe you have appendicitis and operation will save your life."
"Now listen here," said my father-in-law, "My own father died of mesenteric thrombosis in 1922. Since that time, I have read everything that was ever written on the subject. Have you?"
"Well, no, I haven't, but I have seen a lot of cases of appendicitis, and I think you ought to be operated on immediately."
The old man looked him hard in the eye and waited a minute. And then quietly said, "Very well."
As anyone can guess from the way I tell the story, he had a mesenteric thrombosis in his belly when the surgeon opened him up. And he was dead before my wife, his new grandson and I arrived to be at the bedside.
Looking Beyond Cheap Oil
It can't hurt if we stop global warming, and probably, in the long run, it will matter more than whether the Jews defeat the Arabs, or vice-versa. However, we won't think so if one or the other blows us up. Timing the sequence means it may be important to settle the terrorist issue, sooner.
Frederick Mason Jones,Jr. 1919-2009

|
| Mason Jones |
Classical music, however else it may be defined, strongly implies music played by an orchestra, or at least a group of musicians. It thus should be no surprise that the members of a famous orchestra bond together for most of their lifetimes in a sense far beyond the ordinary meaning of teamwork. If you are good, really, really good, you will come to the orchestra as a boy, devote every hour of every day to the orchestra, and step down only as a famous old man when you sense that reaction times have slowed. You sit together, travel together, rehearse together, and talk a language of detail which no one else can fully comprehend. Mistakes that one of you made forty years ago in performance, are still joked about because your colleagues know you still feel the pain of it, just as they share their own infrequent but no less fully remembered, moments of failure, largely unnoticed by the audience. When one of your colleagues dies, you turn out by the hundreds for the funeral. And when the hymns are sung, the organist is ignored, struggling to keep up with the people who really know music.
Mason Jones attended the Curtis Institute, itself a collection of prodigies, and was hired by Ormandy after a single audition; a year later he took the position of a first horn and kept it until he finally sensed he was passing his prime and laid it down. He was featured in the many recordings which defined the orchestra, and the Philadelphia Woodwind Quintet. He sometimes recorded as a soloist, but he thought of himself as an orchestral horn player, teaching orchestral horn at the Curtis to many generations of aspirants. He even conducted a little, usually in small groups. His comment on that was that it doesn't take much to be a conductor. "Just ask any orchestra player." At his funeral, it was related that the second horn once had two solo passages repeated within a larger piece, but when its time came there was silence. The second time around, it was played faultlessly. Afterward, Mason was asked what happened. "Fell asleep," he answered. And the second time? "I just played it for him."

|
| St. Peter's in the Great Valley |
Mason's funeral was held at St. Peter's in the Great Valley, illustrating that strange combination of artistic prodigies with modest beginnings, and the highest of high society, who mix together to create a great orchestra. A very well-groomed lady was heard to remark that this was where she had her coming-out party. St. Peters was founded as an Anglican mission church in 1700 in the Welsh Barony, built a log cabin church in 1728, replaced it with a little white jewel of a church in 1856, and added new buildings in the past few years to accommodate the population growth in the valley. The church has abundant well-tended land, sited on a hilltop surrounded by high hills, quite suitable for a college or private school campus. The homes in the area are a step beyond splendid, hidden in the wooded countryside. Unless you know precisely where to go, the tangle of country roads will defeat you. But the arterial of U.S. 202 is only a few miles away, and Philadelphia's silicon valley nestles beside the highway, inevitably closing in on the countryside. There will be horses and kennels and fox hunts in the region for another decade perhaps, but the new world is moving in on the old one, from all directions.
The Godfather
|
| Angelo Bruno |
{kind=link}
There are people who deny that Philadelphia has any organized crime; and it certainly doesn't have a Mafia. That may be true, but still the rumors do persist. They say in the street that someone named Angelo was once the head of the mob, and that may not be true either. However, it is true that one day he had his head blown off sitting in his car, and it is definitely true that the sidewalks were swept and completely safe for several blocks around his South Philadelphia house. If there was an empty parking space along that block, no one took it.
{kind=link}
One day before he met his untimely end, he was a patient on the seventh floor of the Pennsylvania Hospital, and the patient in the next room was a ninety-six-year-old starchy matron, whose faculties were a little impaired, and who had a daughter named Mary Stuart. As commonly happens with old ladies at sundown, one evening the matriarch became a little confused, and shouted out, "Mary Stuart!" After a brief pause, she repeated, "Mary Stuart, Mary Stuart!" This continued for an hour, and finally, Angelo put on his bathrobe and came around to see what was going on next door.
When he appeared at the door, the old lady sat bolt upright and said, "Young man, just who do you think you are?"
Angelo smiled broadly and replied, "Why, I'm Mary Stuart."
Copy of The Godfather 10/11/18 11:09 pm
|
|
| Angelo Bruno |
There are people who deny that Philadelphia has any organized crime; and it certainly doesn't have a Mafia. That may be their view of it, but still, the rumors do persist. They say in the street that someone named Angelo was once the head of the mob, and that may not be true either. However, it is true that one day he had his head blown off sitting in his car, and it is definitely true that the sidewalks were swept and completely safe for several blocks around his South Philadelphia house. If there was an empty parking space along that block, no one took it.
One day before he met his untimely end, he was a patient on the seventh floor of the Pennsylvania Hospital, and the patient in the next room was a ninety-six-year-old starchy matron, whose faculties were a little impaired, and who had a daughter named Mary Stuart. As commonly happens with old ladies at sundown, one evening the matriarch became a little confused, and shouted out, "Mary Stuart!" After a brief pause, she repeated, "Mary Stuart, Mary Stuart!" This continued for an hour, and finally, Angelo put on his bathrobe and came around to see what was going on next door.
When he appeared at the door, the old lady sat bolt upright and said, "Young man, just who do you think you are?"
Angelo smiled broadly and replied, "Why, I'm Mary Stuart."
COPY of Mary Stuart Blakely Fisher, MD 10/11/18 11:22 pm
Working as a woman doctor in the days when women were limited to 10% of the admissions to many colleges, and often excluded entirely, Mary Blakely graduated first in her co-ed class at Binghamton (NY) High School, followed by first in her class at Bryn Mawr College, and the first in her class at Columbia University's College of Physicians and Surgeons. In fact, she had the highest grades in five years at Bryn Mawr and was selected as a medical intern at the Massachusetts General Hospital, going on to the nation's most prestigious radiology residency under Ross Golden at Presbyterian Hospital in New York, and subsequently with Aubry Hampton. During much of that time, she lived in Philadelphia and commuted on the train to New York. She had married me a year earlier, and the train conductor grew visibly more anxious as she became increasingly pregnant during the several-month commute from Philadelphia's Broad Street Station to Penn Station in New York. Both railroad stations have since been torn down, and the baby she was carrying has been retired for ten years after being Managing Director at Morgan Stanley.
The State of Pennsylvania required a rotating internship, and while I still believe that is the best sort of internship, it was particularly galling to have the reason given that her internship was the reason for refusing to grant her a Pennsylvania license. So she got a job at the Philadelphia Veteran's Hospital, and later at Philadelphia General Hospital, the City's charity hospital of three thousand beds. Well, she never mentioned this Philadelphia affront to a premier academic Boston institution, but I didn't. Perhaps church politics are more vicious still, but this little episode illustrates how very nasty medical politics can get. Perhaps it is a feature of the human personality everywhere, but some situations freely tolerate it, while a few others just don't.
Well, in time she was offered the chairmanship of just about every Radiology department in Philadelphia, and turned them down, saying she didn't want to be chairman of any department. Perhaps she meant any department in Pennsylvania, but she never did make her feelings known. Eventually, she did become Professor of Radiology at Temple University, where she happily taught the residents for many years, during the course of which she was given the Madam Curie Award, the Lindback Award, and various other honors. She had an amazing facility to start dictating reports on x-rays before they were completely out of the envelope and always won the interdepartmental contest for diagnosis of strange films, to the point where other, mostly male, radiologists were afraid to compete with her. She won the Lindback Award for Excellence in Teaching. I used to say I didn't know whether she was any good or not, but I never met a radiologist who wasn't thoroughly intimidated by her ability to make a strange diagnosis at a glance. All her life she got along with five hours of sleep, invariably getting to bed after me and getting up the next morning before I did. Essentially, there were twenty-eight hours in her day.
So it wasn't just radiology where she excelled. Her father once told me there was nothing she could turn her hand to, where she didn't excel. Especially female skills. She was past the point of competing with males and beating them, but female skills were something else. She was a master cook, a demon housekeeper, a champion seamstress, a masterful dinner partner. Athletics were never attempted because she knew very well that men hate to be beaten at golf or tennis. It was the era of Kathryn Hepburn and Grace Kelly, and with a minimum of makeup, she turned heads where ever she went with that Bryn Mawr look about her and her painfully simple clothes. Several of my classmates, usually from Princeton, was struck dumb by her looks. For example, my book editor from Macmillan had a classmate of mine for his doctor. That Park Avenue physician never married and confided to the editor that he had been carrying a torch for her, all his life. It brought to mind the boastful lines from Congreve, in The Way of the World:
"If there be a delight in love, 'Tis when I see, The heart that others bleed for -- bleed for me."
The Philadelphia Delegation to he Pennsylvania Medical Society I
THE PHILADELPHIA DELEGATION TO THE PENNSYLVANIA MEDICAL SOCIETY - I
George Ross Fisher, Chairman
Barbara Shelton, Vice Chairman
During the 1988 meeting of PMS at the Adams Mark Hotel, the Philadelphia delegation directed its chairman to write articles for Philadelphia Medicine, describing delegation activities. Many members of the society do seem to have relatively little idea of the activities of their elected representatives, and perhaps need to know more.
The Republic of Medicine
The best way to describe the medical society "system" is to see it through the eyes of a member who, for whatever reason, becomes actively involved in social activities after a variable time as a relatively passive member. Most newcomers to active participation in "organized medicine" are surprised and pleased by flood of insight into the unexpected brilliance of the creators of the system. The central ideas of organized medicine came from two main two sources, the creators of the national constitution in 1787, and the physician group of 1847 who adapted the national constitutional process into a republic of physicians. Both groups met and conducted their work in Philadelphia. No doubt the similarities between the national constitutional system and the Republic of medicine were increased by meeting in the same city, sometimes in the same buildings. Undoubtedly, successive generations of newcomers to organized medicine are able to navigate its complexities by encountering familiar landmarks of national civics. Conversely, it is frequently a source of continuing pleasure to activists in organized medicine to encounter personal experiences which evoke the enduring insights of the founding fathers of 1787.
The Electoral System
Organized medicine, like the United States of America, is not a democracy, it is a republic. What does that mean? It means that all the voting members of county medical societies are periodically asked to select colleagues to represent them. Once elected, those representatives are trusted to make decisions about specific issues on behalf of the members, and those decisions are subsequently binding on society. The general membership generally selects representatives of their own style of thinking, and eventually replace representative's who prove disappointing. The membership makes their views known to their representative is fully delegated to hear the debate and use his best judgment on behalf of those who elected him. In Pennsylvania, delegates each represent about a hundred members of the county society, although in New Jersey there is a delegate for every ten members. In California, local groupings of physicians select their own specific representatives. In Pennsylvania by contrast, the members of each county-wide vote. Collectively, those delegates become the Pennsylvania Medical Society House of Delegates collectively select about one-tenth of their number to become delegates to the American Medical Society. Since few medical issues markedly separate Pennsylvania's viewpoint from that of the rest of the country, delegates originating in Pennsylvania are representative of the profession as a whole more than they are agents of local faction. Similarly, few issues before the Pennsylvania House of Delegates evoke a special Philadelphia viewpoint.
From this overview it can be seen that any physician who wants to be presidents of the American Medical Association need only persuade a few of his friends to vote for him as a delegate to the State Society, then persuade about a hundred of his fellow delegates to make him a AMA delegate, and subsequently persuade 201 of the other AMA delegates to elect him president. Many doctors from Philadelphia have climbed this ladder, and every doctor who reads this article could potentially do so. Of course, it turns out to be a more difficult path to follow than to describe, but perhaps this oversimplified description will serve to illustrate the vital essence of a republic: selection of representatives at each step is always in the hands of a small group of electors with opportunity to know the qualities of candidates intimately. No television "sound bites", newspaper posturing, or demagoguery from a podium will elect someone well known to the small group of peers who cast the ballots. No candidate within such small groups can long conceal major personality flaws or biases from the group. Sometimes someone claims the leadership of medicine does not reflect the viewpoint of the rank and file; it is hard to see why that should ever be so.
The Republic of organized medicine derives from elegant design, but it contains one potentially serious flaw at the very beginning step of the process of election. The individual physician members of many country societies mostly do not cast their ballots. From many conversations with members, it is clear that the main source of failure to cast votes s not indifference or inertia, but rather a fear that lack of information will inadvertently lead to a vote for the wrong candidate. A system which was consciously designed to assure that voters really knew the delegates for whom they were voting can thus sometimes fail because a high conservation electorate fears that its information is inadequate. All information is only partial, but the individual physician's assessment of the fellow members of his hospital staff or neighborhood is surely superior to the knowledge available to voters in any other sort of election it is possible to name. The society can be positively assured that the scrutiny of candidates once they become active in organized medicine is intense, but it is entirely up to the membership to be serious about choosing local captains.
The Caucus System
Historians relate that the founding fathers of the American Republic did not anticipate the development of the party system, which was largely the creation of Martin Van Buren. That is, the founding fathers did not anticipate that coalitions would form among voters with enduring special interests related to geography. The Republic of medicine has never developed a party system, presumably because the members of a single profession have fewer reasons to polarize for more than a vote or two. Coalitions definitely do form, but seldom endure for more than a year or two before some other issue causes new coalitions to reorganize. However, the large volume of business creates a need for small discussion groups, and group efforts are required to promote the election of officers of a profession which unite and inflame the passions of a geographical locality against some other region or locality. Mostly, however, state and regional caucuses are study and discussion groups, social clubs, and mechanisms for promoting the election of members who are wise enough to know that intense personal ambition is not a highly regarded quality. Although passionate love of your hometown is a faintly ridiculous component of a professional scientific society, there can be little doubt that the local caucuses operate to the advantage of the profession by identifying and encouraging useful leaders who might otherwise be too diffident or awkward to succeed on their own. By promoting its obligated members to leadership positions, the caucus puts its stamp on policy; the reelection process then ensures that those in leadership positions will return to their grassroots with information about "inside" activity. Caucuses provide instruction for newcomers, an opportunity for young delegates to select informal mentors at the breakfast tables. And caucuses give some entertaining parties, which greatly relieve the tedium of a great volume of detailed professional business.
The Reference Committee System
Reference Committee are a particular invention of organized medicine. They are not to be found in the United States Congress, or in Thomas Jefferson's American modification of the rules of the British Parliament, or in the famous rules of order written by General Roberts. The inventor of reference committees at some early House of Delegates of the American Medical Association is apparently not discoverable, but the high priestess of parliamentary process today within organized medicine is Mrs. Sturgis. Her book describes the process of the speaker of the House convening select member committees to review privately the complexities and merits of business before the House, capsulize their opinion, and present it before the fully assembled House as respected advice for general consideration in the debate. Her book also leads the parliamentarian or the speaker around most of the traps and inconsistencies which have surfaced during decades of use, setting sensible rules which mainly allow the assemblage to avoid entanglement in its own processes.
The reference committee system is essential if we are to preserve the right of every member to submit his complaints, suggestions, and resolutions to any meeting of the House of Delegates. The system makes it possible for any member of the society or invited guest to deliver written testimony, or to speak before a microphone without any time limitation. At the same time, the reference committee system makes it possible for a House of Delegates to vote as a whole on several hundred issues in a session, and to be satisfied that their votes were informed ones.
Different speakers have different views about the composition of a reference committee; and different houses of delegates have differing traditions. Currently, the American Medical Association follows the traditions of assigning each member of the House to reference committee in rotation, a system which places a member on a reference committee every eight or ten sessions. An effort is made to assign members to a committee covering subject material with which he is not strongly identified, and hence is likely to give neutral impartial opinion. At the Pennsylvania Medical Society House of Delegates, there has been a tendency to pick reference committee members with a great deal of expertise in the subject under discussion. There is something positive to be said about both approaches. There is nothing sacred about the opinions of the reference committee, and many of their recommendations are swept aside by the House. Consequently, a reference committee chairman quickly develops the goal of providing advice which he believes the House will accept, thereby avoiding the embarrassment of a snub. The reference committee system is to some extent an elegant mechanism for harnessing the egotism of the committee members to the goal of reducing unnecessary floor discussion and quickly achieving the will of the House. Those who are ignorant of Mrs. Sturgis' rules quickly find the pace of business leaves them and their favorite projects behind.
The AMA has the perfect vehicle for defining the quality of care in a particular situation, the PRO system has the people on the front line, observing the gray areas and problem areas. The overlap delegates Weeks, Pierson, Eberle should hustle up the others to forward a stream of requests to AMA to study particular areas. The outcome should be that the collected works of CSA would become the de facto standard for quality.
Subject: Washington Fellowships for Doctors
The Robert Wood Johnson Foundation supports six fellows in health care each year; Allen Hyman was one. The PMS or AMA ought to establish an office for locating suitable candidates and finding fellowships for them. Roger Egeberg suggested as his person. Cost limited to the expense of putting the deal together; the fellowship money to come from foundations. White House fellows, Johnson fellows, Pew fellows, etc.
Lay Oversight of Physician Orders in Intermediate Care Facilities
Whereas, federal regulations concerning intermediate care facilities (400.150) specify (E),(2) that drugs for the control of inappropriate behavior must be approved by the interdisciplinary team.
And Whereas, regulations (483.440) specify that (C),(1) each "client" must have an individual program plan developed by an interdisciplinary team which represents the "professions, disciplines or service area which are relevant".
And Whereas, the statute and regulations (1801) declare that "Federal interference with the practice of medicine is prohibited".
Therefore be it resolved that the AMA study all sections of the Social Security Act which utilize the word "client" in a medical setting where the term "patient" might equally apply, seeking to determine whether some regulatory provisions promote interference with the practice of medicine.
How to Cope with a Trillion Dollars of your own Money.
"Eighty years ago any one of the 'tycoons,' whether in the U.S, Imperial Germany, Edwardian England or in the France of the Third Republic, could and did by himself supply the entire capital needed by a major industry of its country. Today the wealth of America's one thousand richest people, taken together, would barely cover one week of one country's capital needs. The only true 'capitalists' in developed countries today are the wage earners through their pension funds and mutual funds." (Peter F. Drucker, The Wall Street Journal, September 29, 1987.)
In the passage displayed above, a noted authority on the American economy has concisely captured the new dimensions of capitalism in the Twentieth Century, even though his jump in logic can be disputed. It is too soon for the evolution from Nineteenth-Century tycoons into universal capitalism to have affected common parlance; redefinition took place without anyone's planning or prediction. People who describe themselves as workers and employees are slow to develop attitudes and skills appropriate to their new economic power. It is equally uncongenial for those who think of themselves as entrepreneurs and managers to accept "people's capitalism" as the present and growing future of free-enterprise America. Drucker's partitioning of the country into two classes may well be disputed, but he has an insight of some sort which warrants examination. Obsolete class rhetoric will doubtless persist through several more presidential election campaigns.
Two things fit together here. It takes a ton of money to finance a multi-trillion a year economy. It also takes a ton of money to pay for a whole country to retire from work at age 65 and then go on a twenty-year vacation. The new imperative of capitalism is that we somehow must save enough of our collective working income to supply the capital requirements of the economy, which must, in turn, employ such capital efficiently enough to pay for our old age including its inherently heavy medical costs. If we have wars we will have to pay for them too, but the main dividend of our economy does go into a national retirement nest-egg. That's why we work, and that's all we have when we are done working. Stop worrying about quick-rich stories like Mr. Boesky's concerning conspicuous consumption by overpaid yuppies on Wall Street. Forget about the occasional person who takes a year or two off in mid-career to wander around Nepal. Don't however forget to remember the poor, the disadvantaged and the shiftless, because they get old too, and are part of the molten mass. In my view, the national economy can be roughly summarized as a process in which we collectively attempt to have nearly everyone spend his last cent on the day he dies but not a day sooner, living as well as he can in the meantime. Within the scope of this description we thus all become capitalists as we strive to enjoy twenty years without working income after we retire. The only alternative is that we mustn't live so long.
Because broad-based or near-universal capitalism has evolved recently and is not entirely acknowledged, the present system has some large transitional defects. Health insurance, unfunded health insurance, is one of the main defects we will get to in a few pages. A more immediate structural defect is what is that we have not yet evolved an efficient system of aggregating the savings of a nation of little capitalists who are unsophisticated in the ways of Wall Street and want to stay that way. Not only does it cost excessively to hire investment advice, but the voting power of ownership control gets lost in the process.
In the bad old days, when J.P. Morgan and others would buy common voting stock, they bought the company, and the company certainly knew it had been bought. If all of the officers and managers of the bought company weren't soon changed, that was only because they made desperately clear they were ready to take orders about company policy. By contrast, when T. Boone Pickens today buys a similar share of the voting stock of a corporation, the hired hands appear before a congressional committee, or the legislature of Delaware, to get a law passed outlawing the "unfriendly takeover". In Morgan's day, money didn't just talk, it screamed. Today, well, money is in a fight for its life with one-man-one-vote power in the hands of elected representatives. People's capitalism has become a humbled passive investment process, although not necessarily a cheap one, or invariably profitable.
There may be some exceptions, but the middlemen in peoples capitalism have generally declined to grab the voting power which the small stockholder cannot usefully exercise. The people who run what is known as the "Institutions" are custodians of great gobs of other people money in a mutual fund, pension or insurance trusts, and hence hold enormous voting power in the election of corporate directors, officers, and auditors. For some reason institutional investors seldom vote against the management, generally preferring to sell the stock if they are dissatisfied with the way things are going in a portfolio company. Consequently, the entrenched management of major publicly held corporation can do just about as it pleases even following policy disasters. To say this is a flaw in our system is a massive understatement. Things which run by the law of gravity generally tend to go in only one direction. No one wants to see the Japanese pulverize our major corporate jewels, no one wants to see them repeatedly greenmail. Nobody loves a corporate raider.
And still, it is clear the little stockholder cannot and never will aspire to meaningful voting power in a corporation which has millions of shares and thousands of stockholders. (Footnote; When I get those expensively packages proxy cards for my pitiful holdings, I always vote along with management. My theory is it's a good thing to change watch dogs frequently, and my Quixotic vote might hurt somebody's feelings enough to notice the message it sends). The system of governance of very large corporations needs to be reformed by its insiders before consumer activists using one approach, or elected public officials using another, manage to fill the power vacuum to our national disadvantage. They might, for example, reexamine the New York Stock Exchange rule, prohibiting the listing of companies with more than one class of stock. Someone should be asked to evaluate the experience of companies like Ford which evaded the rule, or of those companies which escaped to other exchanges to avoid it.
The directions such reform might take are not the concern of this book; the present focus is on the difficulties which are created for pre-funded health insurance by the fact that corporate voting power materializes whenever major purchases of common stock are made for purely investment purposes. Unpredictable things happen no matter how the stock is voted. If the voting power in the hands of custodians is never exercised, corporate control automatically concentrates in the hands of those whose ownership is relatively minor, whether insiders or outsiders.
One does not have to be a rabid conservative to recognize that government ownership of voting control of a corporation is a form of is w form of nationalization. The Labor party in England nationalized the steel and airline industries, the Socialists in France and India nationalized the banks, Communist doctrines go to the extreme of requiring government ownership of the total "means of production". If we are imaging success in the effort to pre-fund a trillion dollars of health insurance, we have to contemplate the highly undesirable features of potential government control of the voting stock of IBM, American Telephone and Telegraph, Exxon, and Morgan Guaranty Bank. The aggregate worth of all he stock on the New York Exchange is xx xxx. A trillion dollar worth of all the stock implies voting control of quite a bit of corporate America, no matter how sincerely its managers try to avoid it. a resolutely passive investment stance would just make it cheaper for the Japanese to buy control or for that matter the Russians, if they wanted to do it.
This scary line of thought potentially leads to the conclusion that pre-funded health insurance should avoid the purchase of common stock. But that seems bizarre; the historical difference between a 3% return (bonds) and 8% return (stocks) means this voting control issue could condemn health insurance pre-funding to a pitiful fraction of its potential for reducing the costs of an essential social service. It seems imperative to seek ways to improve the long-term return, even if government-controlled pools have to be rejected. True, massive increases in the proportion of non-voting stock confer unwarranted power to the management of the corporations and their potential greenmailers, no matter who runs the passive investment pool. Go one long jump beyond that; they just cannot be permitted.
As a matter of fact, it is impossible to conceive of a permissible investment vehicle for a government-controlled fund, except government bonds. Unfortunately, when you look at what has happened to the Social Security trust funds which are totally invested in government bonds, you find an appalling thing. Buying government bonds isn't too satisfactory, either.
When sums approaching a trillion dollars are involved, even the finances of the United States Government must reckon with the law of supply and demand. If a lot of people want to buy government bonds, they push the price up as long as the supply is limited. Since government bonds are issued to pay for federal debt, increasing the supply of those bonds means increasing the national debt, so we ordinarily don't want to do that either. That is, we don't want the Treasury to issue more bonds just to provide a safe investment vehicle for funded health insurance. On the other hand, by restricting permissible investment to government bonds in huge amounts we cripple the cost reduction of health insurance, since the inevitable result of clamoring to buy bonds will be lower interest rates. Quite aside from the fact that a captive customer gets shabby treatment, it may not be in the national interest to lower interest rates. Since Government bonds are regarded as the safest possible investment, their rate is the floor under all interest rates in the country or even the world. So, lower interest rates are inflationary, even at times when it may be contrary to national policy to stimulate inflation.
What this focus on government bonds has stumbled onto is the mechanism by which modern government attempt to fine-tune the national economy, a process mostly devised by the British economist Maynard Keynes. Based on the premise that no one controls enough money to affect the market price of government bonds, the government sets the price by buying and selling to itself. This particular conflict of interest operates between the Treasury which issues the bonds, and the Federal reserves which buy them. To a certain extent, the Arabs and the Japanese have been rich enough to influence the price of US Bonds, but the largest "external" bond buyer has been the Social Security trust funds. The quasi-external quality of the trust funds is often minimized or exaggerated as it suits some momentary purpose. If more money flows into the funds from tax payments than flows out for pension checks, the trust funds are described as assisting the national deficit. However, if the future indebtedness of the funds is increased more than current revenues are, this debt is regarded as the trust funds' problem and not a matter of national accounts. All this is a cross-generational difference in point of view. My generation can only see it as one big sticky ball of wax. The Federal Reserve's regards it as a major obstacle to their effective use of Keynesian principles. One has to conclude that it would be very unfortunate to add a great big lump of health insurance funding to a government bond problem which will be convulsive enough without it.
In summary, what can we conclude about investing the proceeds of funded health insurance, if we could ever get around to funding it? We see that the creation of a new source of investment capital would be an enormous asset for the national economy, but reckless dumping of huge amounts of cash in any market at all could be disruptive. The purchase of common stock would be considerably more cost-effective than buying bonds, and in the long run, might even be safer. However, equity markets need to consider how to cope with the continuous concentration of voting control of major corporations by default, as a majority of votes would become further locked into passive custodial accounts by funded health insurance. And finally, control of funded health insurance by government agencies poses the same problem of stock voting power which is left to Wall Street to solve, the next chapter tries to consolidate these issues into a general prescription. Remember, Index fund investing is momentum investing. If everyone does it at once, it will pop the bubble.
Four Prescriptions: Proposals or Reform of Health care Financing Rx. I: PRE-FUNDED HEALTH INSURANCE
The Chicago Quartet Volume Two
Four Prescriptions: Proposals or Reform of Health care Financing
Rx. I: PRE-FUNDED HEALTH INSURANCE
INTRO page 1.
Introduction
Benjamin Franklin organized the first American fire insurance company in 1736. Success in the insurance business rests almost unnoticed among the many scientific and political accomplishments of that remarkable man. Even in Philadelphia, few people realize Franklin’s company and several others like it still operate comfortably. Franklin called his company a “Contribution shipâ€, but a more familiar modern term is “mutual†insurance company. Even though mutual life insurance companies have come to predominate, for important reasons fire insurance has been more salable when provided by profit-making companies. The ancient mutual fire insurance companies remain small but reflect some important thinking which this book argues should be applied to health insurance, where ideas are currently badly needed.
What the world already knows about these quaint little companies is almost a hindrance. Occasional articles in the Philadelphia Sunday supplements do sometimes mention them, mostly fascinated with how socially prestigious it is to be a member of their boards of directors, what excellent dinners are served at directors meetings, what priceless antiques are to be found in their headquarters. Franklin to be sure would probably relish the elegance. Unlike the Quakers of Colonial Philadelphia, Poor Richard was not frugal in order to be inoffensive; he was frugal to get rich. Dying the second richest man in the city, he lived the kind of life many Yippies might admire.
Mutual fire insurance companies sell something called "perpetual insurance" which turns out to be perfectly ordinary homeowner's insurance, with one big twist to it. The customer makes one large lump sum deposit in advance, then never pays premiums. During all the time the insurance is in force, perpetually if need be, no further premiums are paid. The deposit earns enough interest to pay the full premium cost of the insurance protection. In that way, the customer has the perfectly astounding experience of having every penny he paid to the company returned when he eventually gives up the insurance. Centuries of experience show that a single deposit of roughly ten years conventional premium will generate enough investment income to cover all anticipated costs from "losses" and administration. The deposits themselves "share the risk", eliminating the cost of paying investors to provide a "contingency reserve". This simple scheme is Perpetual mutual insurance.
As everyone knows, that isn't the way most fire insurance works; the only things perpetual about a more typical policy are the yearly premium notices, which in the aggregate eventually cost much more than making a deposit and giving up the income from it. It is left to the typical stockholder company to worry about getting contingency reserves coming from investors are more popular with homeowners than reserves they have to provide themselves, consequently why perpetual premiums are so much more scalable than perpetual insurance. The young homeowners is typically a debtor, stretching to buy the best house he can afford when he can stump up a down-payment; fire insurance is something his mortgage banker insists he buys. In order to have the American dream a little earlier, the homeowner agrees to pay a little more, later.
Two hundred years after Franklin's death it is possible to gain other insights from "perpetual" insurance because the unfamiliar approach makes us ask basic questions. The next several chapters of this book now set out to argue that health insurance has some serious problems which could be improved by asking those questions. The problems of health insurance are not trivial; many experts question whether we can afford to continue the present system. Whether a breakdown of health insurance would lead to worse care, no access to care or rationed care, the whole subject of health insurance is important to more people than insurance executives. We will return to Franklin's idea after a flyover of current major problems of health insurance, with reflections on how things got to be such a mess. Then, after compounding several insurance remedies based on Franklin's formula, an effort is made to identify potential harmful effects but few are found. The main problem with the prescription is that it has a rather bitter taste.
WHAT'S WRONG WITH HEALTH INSURANCE
There are many things good about the American system of health insurance. Compared with the nationalized health insurance schemes of other countries, our health insurance is a utopia. Indeed, the main reason to criticize the American system of health insurance is to save it from itself, since the foreign alternatives are so much worse. No doctor ever saved a patient by ignoring the symptoms. To be concise, our health insurance system is unfunded, inappropriately linked to employment, adequate for moderate illness but not for catastrophic ones, and incredibly expensive to run. For each of these four disorders, this book offers a prescription. In the first section, keeping Poor Richard in mind, the disorder under examination is that health insurance is unfounded. For the ailment of being unfunded, the prescription offered is the IRA for Health.
Unfunded, Being unfunded does not mean cheap. It costs a typical family about $3500 a year for health insurance premiums. It has become commonplace to read newspaper articles announcing or predicting 15-30% increases. Annual national costs of healthcare are about $500 billion. Those who would like to solve the problem with a national health scheme should remember that $500 billion would be half of the current Federal budget; the $200 billion already federalized are nearly destroying the government. Health care is expensive all right, and unfunded.
Further, because an employee can escape income taxation on a health insurance premium if his employer pays it for him, that's the way health insurance.
One More Idea, Please
The 1975 annual meeting of the Association of foundations for Medical Care was, as usual, a provocative and informative forum for mutual exchange of ideas. An entire day was devoted to exploring the problems which need to be solved in order to get an Independent Practice Association off the ground and solvent. How do you attract subscribers? How do you enlist the support of physicians?
One disturbing problem was not resolved, however, and the failure even to discuss possible solutions seems even more disturbing to me. That problem is this: what mechanism will be devised to set fair medical fees if your IPA should be so successful that it enlists every physician and sells every subscriber? That is, how do you anticipate the problems of a monopoly? While it is understandable that the potential problems of success are swept aside at a time when the immediate problem is to achieve a viable toe hold, it would be tragic to allow the time of formative philosophy to pass without the setting of goals.
Our fees are now set by the marketplace. As Adam Smith remarked, if you charge too much you lose to your competitors, and if you charge too little you will go bankrupt. The price of everything, Adam Smith said, is therefore always fair and right in a freely competitive market place. The fees of an insurance mechanism are therefore also fair and right if they are "usual and customary". The strong implication of that little phrase is that somewhat a competitive market exists as a standard.
In Pennsylvania we are peculiarly in a position to see what happens when a good hearted idea like Blue Shield becomes so successful that the market place disappears. What happens when you destroy the marketplace is that fees are set by committees, later demand to be a majority of the committee, and eventually demand to exclude physicians from the committees entirely on the argument that the foxes should not be watching the hen house. Frustrated by skillful insistence on charter and by-laws, such customer groups then resort to a different approach: They apply political pressure on the Insurance Commissioner to deny permission for premium increases. This whole process can be summarized as substituting the political process for the market mechanism. There are, after all, more patients than doctors, and this distortion of the marketplace inevitably leads to downward pressure on fees. If you accept Adam Smith's dictum that fees set by the market mechanism must have been fair, it follows that this whole shift leads to fees which must be unfairly low.
Well what do we do about this? First, let us acknowledge one left-handed fairness to it. It is very noticeable that there is no movement at all for IPA's are concentrated in the medically overserved areas because they almost invariably develop as an opposite reaction to closed-panel group practices in their areas. The whole pre-API movement has a suspicious look about it of having no genuine concern about pre-payment, but rather the motivations of a consumer cooperative movement. It is hard to know what to think of this. It certainly does add a disincentive to practice in overserved areas, and probably causes a certain number of outraged physicians to migrate to underserved areas. However, to the extent that physicians are willing to accept less income in order to have the other advantages of living in the suburbs, it can be expected that the total cost to the overserved community will remain the same or rise if the physicians surplus is reduced. Therefore, in the long run, the effort of starting HMOs is self-defeating financially except for those consumer power groups who can take special opportunities for themselves. The other less forward consumers will find themselves with fewer physicians availability, at higher costs.
To return to the problem of preserving a market mechanism for the establishment of fees, several ideas seem worth considering:
1. Limit the market penetration of any group to 20% of the market in its area.
2. Require that no group may exceed a 10% market penetration unless at least four other groups are genuinely competing with it.
3. Identify one whole specialty of medicine as excluded from the "total" coverage of the insurance plan, and use this free-enterprise specialty as a reference group for fees of other specialties. The relative value system would expand from this base.
4. Never start an IPA unless a closed-panel program exists in the area.
There are a number of unpleasant or demonstrably ineffective measurer which could be tried.
5. Limit physician income to a "reasonable" level.
6. Deductible and coinsurance.
THREE WAYS TO ACHIEVE FUNDED HEALTH INSURANCE
Since everybody would benefit if the country found a way to pre-fund health insurance, what options are available or doing so? Or put another way, what obstacles, objections, and vested interests obstruct each possible way of doing it; how difficult would it be to overcome them?
Three general approaches might work reincarnation of Individual Retirement Accounts (IRAs) .for this special purpose, the legal encouragement of health insurance companies to sell permanent insurance or the creation of a national trust fund. Each of these approaches will now be changed to make them possible. All of them must somehow overcome the main problem inherent in payment in advance, which is that people must find spare money somewhere. while of course the disposable income could be found by reducing expenditures for non-essential luxuries, this discussion limits itself to examining how seed money might be squeezed out of inefficient practices in the existing health financing system.
Health Banking The first approach to be examined has been known by several names. When Michael J. Smith of Louisiana proposed it, he called it the CHIP proposal (Consumer's Health Investment Plan). When John McClaughry and I independently proposed something similar, it was called the Health Protection Account, Peter J. Ferrara of the Cato Institute, who likewise got the idea independently, had the genius to call it the IRA for Health. The IRA for Health has the great beauty that the title itself does most of the explaining; most people know what an IRA is, or was. An IRA for Health is obviously an IRA whose use is limited to health care costs. Unfortunately, congressman, whose cooperation is vital to the success of the idea, have gone through the experience of repealing the tax exemption of IRA's trying to reduce the national budget deficit. Congressmen have the mindset that IRAs will worsen the deficit, or at least that their constituents might think so. It isn't a correct perception, but the catchy H-IRA title has become a hindrance and must be replaced. Health Banking is here offered as a substitute title for Health Iras because it suggests an interest group who might assist the process of public persuasion because they would benefit from it. The definition of what constitutes a bank is in the process of change; perhaps there is room for health banking in some future compromise revision of the Glass-Steagall Act. For example, the mutual fund industry could become interested in health banking as part of their vision of non-bank banking. Perhaps the moribund savings banks could be entrusted with a trillion-dollar consolation for their regulation-induced troubles.
Whatever institution might aggregate and invest the funds, the main idea is that the tax-sheltered money which employers now spend on health benefits would be deposited in individually named accounts, and invested according to some rule of prudence. Withdrawals from the accounts would only be permitted for specified health purposes. It is absolutely central to understand that nothing is here proposed to be tax sheltered which is not already tax sheltered. For better or worse, employer contributions for health benefits are already tax-sheltered, and will almost surely remain so. Even recent deficit-desperate congresses have not dared to threaten that $50 billion annual revenue cost to the Treasury. Indeed, when Congress does develop the courage to curtail the tax exemption of health benefits (for employed people), perhaps then health banking could be described as costly. Until such time, however, it remains fair to generalize that reestablishment of IRAs, limited to health expenditures, has no Federal cost.
In the next chapter, we will discuss the investment issues which are raised. For the present, we should assume that the institution which becomes custodian or health banker will generate a safe and adequate stream of revenue; what rules must govern the way it is spent? Ideally, a health investor would want to accomplish the following goals:
-He would want to pay for essential health care.
-If he lives a long time and has money to spare, he would want to provide for custodial care in his old age.
If he dies and has money left over, he would want it to go to his estate.
But these are decreasing priorities. The first rule is survival. If he cannot pay for his old age, he must plan to throw himself on the mercy of family, friends, and community. If he has nothing left for his heirs that is no worse than a pity when he has no dependents, but tragic if he does.
To the foregoing self-evident principle should be added two more which are less adequately appreciated. The first is that the federal government has long addressed the problem of aid for dependent children, and ordinary Social Security benefits are quite generous for survivors. No doubt these programs for widows and orphans could be more generous, but they are as generous as twenty congresses have decided to be; it is unrealistic to include provision for dependent survivors in a new program proposal.
The second mitigating principle is nature's trade-off. Nothing is more clear to a doctor than the experience that ten percent of his practice develop ninety percent of the illness. If you get very sick very often, you need not worry greatly about the prospective costs of living for years in a retirement home. Dying young is a tragedy, and outliving your income in a shabby old age are both tragedies, but relatively few people experience both of them. To the extent that some people are needlessly insured against both disasters, it should be possible to create insurance efficiencies by combining both risks in one funding mechanism.
By reflecting on the general principles of prudent provision for the future, we arrive at the following proposed rules for releasing money out of healthy banks (aka IRAs for Health). Vouchers may be issued, or disbursements made directly, to pay health insurance premiums, front-end deductibles, nursing home insurance, entrance fees for life-cares communities, specially designated trade-offs with Medicare, and payment of any residual balance to the individual's estate. Investment income would not be taxed, but the estate tax would apply after age sixty-five. Since this statement of benefits is technical and terse, the following explanatory footnotes are necessary:
Payment of front-end deductibles. If the health bank only paid the present premiums of health insurance there would be nothing left over to invest. It is anticipated that premiums would initially be lowered y purchasing health insurance with at least $500 yearly deductible, and the amount of the "front-end" deductible would later gradually rise as funds accumulate in the account. This process would, in turn, cause a progressive lowering of the premium of the health insurance, accelerating the savings. When expensive illness occurs, the fund would reimburse the subscriber the full amount of the deductible, upon presentation of evidence that his health insurer had paid out amounts in excess of it.
Special trade-offs with Medicare, Nursing home care, Life-care communities. It will be necessary for the reader to be patient for these proposals to coordinate health banking with the entitlements under Medicare and federal catastrophic health insurance. The subject is dealt with in the section of the book devoted to Prescription II: Last Year of Life Insurance.
Payment of Residuals to Estates.No doubt there would be an instinct to examine whether the program could be made less expensive if residuals were forced to revert to the federal treasury. To permit an estate to retain these funds would seem to enrich the heirs out of funds which were largely made possible by federal income tax exemption. True enough, but long experience in my medical practice with life tenants of trust funds has been that they will relentlessly seek ways to spend money on pseudo medical care if there is no other way to get their hands on what they regard as their rightful money. Some incentive must be created to prevent "health insurance companies" from creating benefits like suntan oil and health spas in warm climates, whose only real purpose is to collude with beneficiaries. To attempt to prevent this sort of behavior with regulations is laughable.
That's not all you could do with health banking, however. If individuals should die young or use up all of their funds with repeated expensive illnesses, they might seem to be about where they are now without health banking, minus the extra layer of administrative overhead. But they have achieved portability. They can become unemployed, change employers, or retire early without the same concern that they have lost their health insurance. If they have developed a chronic problem, it has not become a "pre-existing condition" in the eyes of some new insurance carrier. They can quit their jobs without fear that a new employer with company self-insurance would regard them as potentially expensive employees. They need not fear that post-retirement health benefits will be blown away by a corporate raider, or that the company where they worked for years will subsequently go bankrupt and leave them with empty promises instead of health insurance. Portability.
For the vast majority of participants, however, another whole new concept becomes possible after a few years. We are now back to Benjamin Franklin and perpetual insurance. The health bank was just a transitional stage to reach it. The ingredients of perpetual health insurance are:
The fund has grown so large that its investment income is big enough to pay the premium on a high-deductible health insurance policy without any further contribution
And the fund is big enough to pay all of the deductible portions of a major illness
And there is still enough investment income to pay the premium of a reinsurance policy which covers the unusual instance of sustaining two or more major illness.
As a guess, such a fund would be in the neighborhood of thirty thousand dollars. As a further guess, most people would continue to work past the time the fund went perpetual, and further contributions would accumulate. Individuals who reached this happy state of affairs would almost by definition be fairly healthy, and in all likelihood would look forward to a long and dreadful sojourn in a nursing home. For a quick overview of the situation, the next time you go to a high school reunion, take a stroll over to the area where the fifty-year class is meeting. About half of the class will be in attendance, some in wheelchairs, but the other half of the class will be in memoriam. Fifty-fifty at the fiftieth.
What has been briefly described is a mechanism for designating a considerable amount of funds for long term care that are not now available. It was achieved without financial or other barriers to healthcare access except possibly some self-denial since full reimbursement for healthcare is available to every participant. If someone wants to put up with his hemorrhoids in order to have more money for later nursing home care, or if he wants to hold off entering a nursing home in order leave more money in his estate, well, those are his options. If he holds off getting treated for his cancer "for those same reasons", in my medical experience those wouldn't have been the true reasons", in my medical experience those wouldn't have been the true reasons at all and he would have held off no matter what his insurance arrangement might be. So, what's the magic? Where did this money come from?
From the operation of compound interest of between 3% and 8%, depending on the amount of equity risk assumed.
From self-denial of borderline necessary or even frivolous medical expenditures in response to the development of an incentive to save.
From the downward pressure on medical prices created by a more cost-involved public.
From the out-of-pocket contribution of health care expenses which fail to exceed the yearly deductible amount.
From reduced administrative costs of processing small claims through first-dollar coverage rather than paying them out-of-pocket. The reader is invited to consider this issue in more detail in Prescription IV: Insurance Tangles.
Will all this be enough to carry the project? Hard to know. What isn't hard to know is that savings of just 1% of a $500 million annual medical cost, amount to $5 billion per one percent saved.
Health Insurance Companies Unchained.Observers of the economic scene, especially the Washington political-economic scene, will be well aware that health banking is a proposal from the conservative side of politics. It had origins in the Reagan administration and the libertarian Cato Institute. A staunch Virginia conservative, Representative French Slaughter, introduced a bill (HR 536) along these lines, and he has been supported by the Republican Study Group under the chairman of Representative David Dreier of California. Just exactly because the proposal has this sort of appeal, it has a strong weakness. The idea is strongly rooted in the idea that individuals should make their own choices, even to the point of being allowed to make wrong choices. Individual citizens should be allowed to have their own way with their own money, even if their betters think their choices are not in the best interest of society or even best for the particular individual.
Well, that's just fine, but unfortunately in this instance, it comes up against a pretty big problem. Even when the IRA was available, only 14% of the eligible public availed themselves of it, there were vast numbers of people who had never heard of it. I spent endless hours fruitlessly attempting to persuade several of my secretaries to create an IRA, and even some of my children had to be prodded pretty hard. An executive of one of the largest corporations in the country told me of the dispiriting experience at his company with a 401 (k) plan, which is essentially an IRA. The company offered to match contributions dollar for dollar and conducted a large and continuous education program. This man made the estimate that in the whole corporation no more than a dozen unmarried women availed themselves of the opportunity, and the workforce included plenty of women lawyers and accountants. With an experience of only 14% enrollment in the IRA, it certainly isn't fair to point to just single women as having an anti-saving mentality, although I suppose there is something to it if he says so. In doing my little bit to encourage the world to establish IRAs, I noticed that one of the most effective inducements among those who did it was the wicked pleasure of beating the government out of some taxes.
So, we enthusiasts must make a grudging concession that if health banking is to succeed on a major scale any time soon, it must do more than just make itself available and then wait for everybody to get smart enough to buy it. It isn't necessary to share the rhetoric one union president unleashed on me, "You've got to find a way to keep the working man from spending his wages on drink". The paternalism of that degree is too much for me, but I will concede that something must be done to prod people a little. And that missing ingredient just might be a vast army of glib commission-motivated insurance salesmen.
It must not be assumed that health insurance companies are straining at the leash, impatiently lobbying for legislative release from their inability to sell funded health insurance. In fact, most of them do not have much sales force since health insurance is typically marketed in bulk to employer benefits departments. Most of them do not have much investment portfolio management department, especially outside the area of the short-term paper. There is minimal research on the subject of lifetime health costs. Incentives are weak; health insurance is typically regarded as a loser by full-line companies, Blue plans which dominate what is left are non-profit concerns. Insurance companies are fiduciaries, custodians in trust of other people's money. If careless paying obligations they get sued, if they can't pay their obligations they go bankrupt. If they make big profits they get bad press or ruinous competition, it doesn't matter which.
However nothing important is easy, and we want them to peddle our product. What's their problem? Their central problem turns out to be the fact that funded health insurance asks the company to assume the risk, and no one knows how to price the risk. Using the health banking approach, the individual subscriber assumes the twin risks that future health costs will inflate at a predictable rate and that investment results will equal the historical record. Who knows if we will have inflation like a banana republic, a depression like the one in 1933, or the development of medical miracles no one can afford? That's a risk, which the individual holder of a tax-sheltered medical account might assume willingly on the argument that any outcome could be no worse than unfunded health insurance. Put an insurance company's guarantee into the hands of that person, however, and you had better pay your promise if you want to stay out of court. Life insurance companies are just beginning to experiment with best-efforts investing, using the name of variable annuity life coverage, and that sort of approach would surely be necessary for funded health insurance. Predicting the average life expectancy of a large group of healthy people is however a minor mathematical exercise compared with estimating the aggregate average health care costs for the next thirty-five years. The actuary doesn't even know for certain how many people will have any health cost at all; at least the life actuary knows that everyone is going to die. The advent of a new and fatal epidemic like AIDS shows you what these predictions can be worth. The price Dr. Starzl's hospital charges to transplant your liver startled even me when I heard it last year.
Quick reflection on the issues brings the firm conclusion that health insurance companies could only be expected to offer best-efforts investing, without any insurance guarantee at all. They would surely market the product skillfully, as we desire they should, but the cost increment would be quite appreciable. The sales cost for life insurance is typically equal to the entire first year's premium, while an additional profit must be offered the company to induce it to handle the product. Investment experts will have to be paid to manage the money, and they characteristically value their own services highly. It's too bad to have to say it, but if you are too dumb to manage your own money you are going to pay through the nose to have someone else do it.
Perhaps this is an appropriate time to mention the idea that some large unions have toyed with, of becoming self-insured for the health benefits of their members. All that means is they would expect the employer to give them the money, and they would pay it out. In order words, they propose to become insurance companies. Most everything which has been said about other health insurance, therefore, applies to them, too. In addition, it might not hurt to mention Ricardo's principle of relative advantage, which roughly states that people with professional experience in a field often do the best job at it.
Publicly Managed Trust Funds. The third general method for achieving pre-funded health insurance is one which the American Medical Association as a method for basic restructuring of the Medicare program. In a widely discussed report of the AMA proposed the creation of an independent federal agency to receive the health insurance payroll taxes which now flow into the Medicare trust funds, invest them, and issue vouchers to the elderly which would permit them to purchase private health insurance. The agency would also fill the badly needed role of a group of experts charged with overseeing the course of national health inflation, demographic and health practice changes, and the national investment climate.
The AMA employed expert advice in the preparation of this plan, and it is likely their financial estimates are sound when they project that Medicare could become totally pre-funded by 2016, using tax rates achievable close to present taxation. This plan would include provision for working off the present unfunded liability for existing beneficiaries, honoring commitments previously made to the elderly. It is a great testimonial to the flexibility of the AMA in recent years. as well as to the tremendous power of compound interest, that such a monumental problem could be effectively addressed. After all, the AMA in 1965 quite correctly warned the country that the Medicare program would quickly pile up mountains of unfunded obligations if it adopted a "pay as you go" financing method. Not everyone who has been vilified for being right will subsequently adopt a constructive problem-solving approach to repair the accurately predicted damage.
The creation of an independent board of expert overseers supplies a need which health banking through the IRA doesn't, and creations of a government agency create a guarantor of last resort, even though it might be stoutly denied. Lots of Americans trust their government to keep its promises. However unsophisticated that attitude may be m, it helps get national support for the idea of pre-funded insurance in a way no television spot commercials could do, and no insurance salesman could do over the kitchen table. Every government since the Lydians invented coinage might have remorselessly devalued its currency, and it would not matter. A very large proportion of Americans trust government bonds as they trust nothing else in society.
However, a sizeable group of people simply will not have this approach, and a number of them are in Washington. The AMA made a small tactical error in describing the proposed independent agency as roughly comparable to the Federal Reserve Board in its independence and suggested a similar method of appointment. Apparently, the AMA had no idea of the violence with which the Federal Reserve Board is hated by certain influential members of both legislative and executive branches, or of the decades of bitterness between mid-western bankers and the New York banks which control the open market committee of the Fed. In a sense, the Federal Reserve is actually owned by the banks it regulates and tends to defend their interests. The whole investment community is at war (nice polite war, of course) with banks, struggling for turf in some pending revision of that Treaty of Versailles, the Glass-Steagall Act. Every election year, the Federal Reserve gets embroiled in bitter controversy as to whether its policies are slanted to cover up for congressmen who want the Fed to do their dirty work and have it within their power to abolish the whole agency if it does not comply. Independent as the Fed. Foo.
Let a Hundred Flowers Bloom. No doubt this inflammation can be soothed with diplomacy, but there are more serious worries about the investment difficulties which are unique to a trillion dollar fund run y the Federal Government to be addressed in the next chapter. In the meantime, the three funding mechanisms can be summarized as having certain flaws and certain strengths which are peculiar to each. It seems unlikely that the country could agree to permit only one of them to be designated to the exclusion of the other two. To a serious proponent of the general approach, it seems imperative that we authorize all three approaches while forcing them to remain in competition with each other. After all, we are talking about a system which addresses the needs of everyone no matter how different the circumstances. People who take wild chances should be restrained from becoming public charges, ignorant people should be protected against those who would fleece them. As Adlai Stevenson said, "It used to be said, a fool and his money are soon parted. But nowadays, it can happen to anyone."
There is, however, no certain way to know the future even if you go to Princeton to learn it. Let the banks and mutual funds exploit their lower marketing costs, let the insurance companies sell rings around them. Let the private sector shame the mediocre performance of the public trust fund, while the trust fund stands as a tower of strength among self-serving investment pitchmen. So long as the public is allowed to switch around, things should work out, in an investment version of the system of checks and balances.
Last Year of Life Insurance
Last year of life insurance is life insurance, retrospectively paid after the death of the subscribers to his health insurance company. Although theoretically reimbursement could be made for actual individual expenditures, it is a more powerful idea to reimburse in the amount of the calculated average last-year costs of the community. It could loosely be said this approach constitutes 100% reinsurance of a selected peril, in order to suggest possible variations, such as 105% reinsurance (to transfer administration costs), 80% reinsurance (to encourage case management ), etc.
The last-year-of-life concept should be regarded as a tool for coping with certain problems inherent in the system of basing health insurance on employer groups. Employer-related health insurance is tax-favored, reduces marketing costs, and almost eliminates risk to the insurers; it is far easier to modify such a system than to reform it. However:
Non-random perils like AIDS may cause insurers to withdraw from ensuring particular companies or even whole industries.
Employees who retire early for reasons of health may find themselves unable to obtain health insurance after the COBRA protection period.
There is presently no method available for young people to guarantee their insurability before they enter permanent employment, or for employees of any age to guarantee their insurability in the event of company insolvency.
The risk of losing insurability is present in every change of employment; job immobility is created when fear of health insurance problems is on the employee's mind. Early retirement may be rejected for fear of exposure to loss of health coverage between the time of retirement and the onset of Medicare coverage.
Serious dilemmas for corporate funding of post-retirement health benefits have been created by a fear that voluntary pre-funding such obligations may create cash targets for corporate raiders. An employee has no legal rights to the prefunded reserve even though he may have legal claims for the eventual benefit obligations
Consequently, the most conservative present estimate of unfunded post-retirement health insurance obligation is $100 billion, and it may be four times that.
Since last-year-of-life insurance is life insurance, it might be provided as either term insurance or cash-value insurance. Although cash-value insurance has obvious advantages for the problems listed above, it would not enjoy the same tax-sheltering which term insurance would have, and consequently would require legislative relief to be fully effective. However, term insurance might well offer some relief for the AIDS problem.
Insurers are leaving the Washington DC area because of prohibitions against screening for AIDS, and Massachusetts also has a law against testing. The obvious first resort of an insurer is to withdraw from covering companies involved in the arts, design, theater, etc, and this tendency is paralleled by rapidly increasing detox and rehab costs for cocaine abuse, which have led to harsh exclusions for psychiatric care. The point is that employer-based insurance seldom includes a premium provision for risk, and if a particular peril cannot be excluded then a general class of service or a particular sort of employer is excluded as a proxy for it.
In this particular instance, it is proposed that insurers explore the willingness of their group markets to shift coverage of last-year costs from company-specific to community-rated premiums while continuing to be experience-rated for all other perils. If the various trade-offs were favorable, then insurers might be willing to discontinue offering last-year coverage except through the community-rated life insurance route. At present, the experience is probably insufficient to judge whether a market-driven voluntary approach would be effective. In the event, most companies proved willing to adopt the approach but insurers feared non-compliant competitors who saw an opportunity to steal business, then the public-interest need for legislation to protect the health insurance industry from disruption by the AIDS problem would have to be debated. For those who dislike compulsory solutions, it is exasperating to discover that the insurance industry generally prefers to be compelled by law since to move ahead in a cooperative manner is to invite anti-trust action.
In this particular instance, it is proposed that insurers explore the willingness of their group markets to shift coverage of last-year costs from company-specific to community-rated premiums while continuing to be experience-rated for all other perils. If the various trade-offs were favorable, then insurers might be willing to discontinue offering last-year coverage except through the community-rated life insurance route. At present, the experience is probably insufficient to judge whether a market-driven voluntary approach would be effective. In the event, most companies proved willing to adopt the approach but insurers feared non-compliant competitors who saw an opportunity to steal business, then the public-interest need for legislation to protect the health insurance industry from disruption by the AIDS problem would have to be debated. For those who dislike compulsory solutions, it is exasperating to discover that the insurance industry generally prefers to be compelled by law since to move ahead in a cooperative manner is to invite anti-trust action.
The preceding, or "term-insurance" approach has the advantage of gathering useful information about the last-year concept without requiring extra tax sheltering or even the formality of separate policies or insurance subsidiaries. It could be retrospectively tested on paper without much cost or any risk, and it might be held ready as a potentially useful tool for the eventuality of the AIDS epidemic provoking serious disruption of health insurance. However, much more important benefits might grow out of the cash-value life insurance or refunded, approach to last-year-of-life coss. Since last-year expenses come at the end of a 70+ year life expectancy, the opportunity for compound interest to work is at a maximum.
Under this approach, the initiative would lie with life insurers, who would be induced to include a standard beneficiary clause in their policies. That clause would assign the community-average last-year health cost reimbursement to any health insurance company which had assumed those costs and had previously provided the beneficiary with appropriate consideration for making the assignments. (At the moment, the various secondary adjustments between employer, employee, health insurer, and tax collector can be left to the marketplace to work out. If no one makes an adequate offer, the beneficiary simply has some life insurance).
The cost of such insurance might turn out to be fairly modest. Although average last year-of-life health costs might be guessed to approach $20,000 per death, the comparatively low death rate before the age of 65 means that an average life insurance policy of less than $5000 (with proceeds exhausted at 65) could conservatively be guessed to cover that need. After age 65, every person can reasonably expect Medicare to have a last-year obligation. Using a 65 investment assumption, the present value of such policy would be $250 at birth; a 3% assumption would only be $500 and would allow general inflation the economy to be ignored. (The $5000 figure would seem to allow generous room for potential innate health-care cost inflation, inasmuch as last-year coverage does not require any provision for recovery from one formerly-fatal condition only to die later of a second fatal condition, which is the main cause of "innate" health cost inflation.) Presumably, the best protection against future health cost escalation is to purchase more insurance than is thought to be needed, expecting any surplus to flow into the estate. Even taking a conservative view of the health-cost escalation problem, its possible to imagine premium costs of $100 per year during thirty years of working life.
Although the marketplace could be expected to determine how much reduction in health insurance premium would be accorded for the lifting of last-year risks, the main value of this coverage would appear in the case of someone who was uninsurable (? ie unemployable?) without it, or who would have been afraid to switch jobs without it. When individuals sustain periods of loss of income, the possession of this insurance might be regarded as a form of catastrophic health coverage, which for the temporarily unemployed might be an absolute minimum coverage. The reasoning is that this type of coverage can be switched on or off; a treaty of assignment need only be signed if the individual finds it advantageous to use it, and is later revocable at will. The policy, in short, is his not his employer's but can be made to coordinate with employer benefits.
Medicaid programs are rather dubious candidates for this approach but even they might be induced to be more generous with last-year coverage (probably under either a term-insurance or waiver-of-premium approach) than they have typically been with full health insurance, the becaused potential for abuse is eliminated.
Finally, the relationship with Medicare needs to be explored with HCFA. After all, Medicare is the main health insurers of fetal illness costs. Far from ever escaping these costs, Medicare has a major concern that it may also have to assume long-term custodial and nursing home costs. Far from ever escaping these costs, Medicare has a major concern that it may also have to assume long-term custodial and nursing home costs. In this matter, Nature provides a certain trade-off. Dying young and outliving your income are both tragedies, but few people have both of them. There is a need to consider ways of transferring costs between the two largely-exclusive problems. The aggregate community cost of fatal illness after age 65 is much heavier than it is up to age 65; possibly $20,000 average coverage would be necessary. Since compound interest would have longer to operate, however, the premiums or present-value costs would not necessarily be proportionately larger. A premium of $40 (1988 dollars) could be imagined; there is no reason why premiums could not be inflation-adjusted on a yearly basis as an alternative to making overly conservative interest-rate assumptions.
The proposal is to explore with HCFA he attractiveness to them of providing some degree of long-term care coverage in return for surrender to them at age 65 of paid-up life insurance adequate to cover fatal-illness costs.
QUESTION: If the health insurer agrees to lower his premium, and subsequently pays the last year costs for the subscriber, how can he be assured the life insurance will eventually reimburse him?
Since health insurance is mostly in employer groups, covering only expenses n the current year, the health insurer can limit his concern to the current year. The health insurance annually needs a slip of paper guaranteeing payment by a life insurer, in the event of client death. Three main methods are available, each with implications about who owns and controls the process:
One method is to follow the reinsurance model strictly; the employer pays the health insurer, who then pays a life insurer for "reinsurance". In this case, the health insurer controls the process, which is almost invisible to the employer an employee.
Where the employer already has a group life insurance benefit, he might well wish to send the check directly to the life company for a somewhat larger benefit(simultaneously reducing the payments to health insurer). While this approach gives control to the employer, it also gives him the headache of negotiating the premium adjustments.
Both of two foregoing approaches would be administratively very convenient, but neither one provides the employee with portability between employers, bridging of episodic gaps in employment, etc. For the employee to take advantage of portability, carriers other than the company carrier must be utilized. The employer's health carrier would then need yearly slips of paper from a number of life carriers, most easily obtainable as part of the yearly premium billing process for the life insurance. Such a paper would amount to a rebate coupon, issued by the life insurers, honored by the health insurer.
It is essential to keep paperwork simple for an estimated premium of about $100 a year for a term an $400 a year for cash-value life insurance (of course, only$100 of either would be transferred to the health insurer). Consequently, insurance management would want to look into bulk communication: "Dear Health Insurer, Our records show the following clients have exclusively assigned the average last-year health benefit to your company for deaths which might occur during the period between A and B. Yours Truly, Life Insuror"
Because of the problem of differing premium dates, the insurance industry might further wish to agree on a calendar or other standardized year definition for this type of coverage. The administrative issue can be stated in the plainest possible term: the extra administrative cost of this approach is the price of portability.
QUESTION: No underlying health insurance.
Although an individual with cash-value life coverage could borrow against it to pay health costs, terminal or otherwise, the issue has been raised as to how someone would employ the life insurance mechanism if he did not have any underlying health insurance, but did have term life insurance. Alternatives would be:
He could purchase health insurance with a front-end deductible equal to the face value of the life insurance. MONY sells a $25,000 deductible policy for about $200 a year family premium, with a $1,000 top limit. Such a combination would protect for more than just terminal illness, but it would not protect against more than one heavy cost. For what would presumably be a very low extra premium, he would need another reinsurance policy to cover multiple illnesses. Such reinsurance might have two parts: one part to cover the remote possibility of exceeding the deductible more than once, and another part to cover the deductible on what proved to have been a non-fatal illness. This degree of coverage goes considerably beyond the last illness concept and would naturally cost more.
The main problem with this life-insurance-to-pay-off-the-high-deductible approach is that it presumes the beneficiary would pay his bills in cash and contains no way to spread the risk. Therefore, everyone ends up either overinsured or underinsured. A smaller issue is that he would pay full charges without a way to negotiate volume discounts at hospitals. Taken together, this approach would be unnecessarily expensive.
An approach more narrowly related to the cost of terminal illness would be for the life insurer to pay last-year costs, large and small, but only reduce the net death benefit to the estate by the average community terminal illness cost rather than the actual case-by-case expense. Once the average rate had been established, it would become possible to tailor the insurance coverage, leaving a suitable margin for year-to-year inflation and other contingencies.
The degree to which carriers could pool claims data in arriving at the average cost is an anti-trust question; the definition of a covered expense is purely a question of practicality within claims administration. However, differences of opinion about the feasibility of different coverages might make data sharing less practical.
QUESTION: What if there are multiple carriers involved?
On examination, this question relates mainly to carelessness, misunderstanding or incompetence on the part of the subscriber. Even if the individual has multiple life insurance carriers, he would be foolish to execute a last-year beneficiary clause with more than one of them. Consequently, no such clause should be permitted unless it defines the primary carrier for last-year purposes as that carrier with the earliest date of execution of such a clause which is still valid at the time of death.
With regard to multiple health carriers, the life carrier would generally take the position that he is only going to pay so much, and the health carriers can work it out among themselves. The reasonable division of the award would be in proportion to the degree the health insurers had paid out the actual health costs. No doubt there would be instances of multiple health insurance coverages of someone who dropped dead with no medical costs at all. If the reimbursement were on the basis of average community costs, lawyers for the health companies would no doubt exercise their imaginations in court, but the life insurer would be serene, and the situation would soon clarify itself with case law.
It is somewhat more difficult to contend with the possibility that the life insurance clause would authorize payment of actual individual costs, only to discover that the beneficiary had over insured himself with multiple health carriers, without coordination of benefits clauses. The life carrier would thus be in a poor position to know just what the actual payments by the two contending health insurers had been, and how much overlap or legitimacy there was to them. It follows that the subscriber who requests that individual actual reimbursements rather than average community ones be made, must also be required to specify whether he wants all carriers reimbursed, or only the primary, or only the largest, payor. With the life carrier thus immunized, it becomes the responsibility of health carriers not to reduce their premiums or make other concessions to the subscriber in return for a last-year treaty unless the subscriber can satisfy them that their agreement meshes with the life clauses, or that the subscriber agrees to the coordination of benefits.
Billing Medicare for Office Lab Work (Without Bookeeping Tangles?)
New Law Increased Administrative Costs for Everyone
George Ross Fisher, MD
Philadelphia
Hidden in the hundred of pages of the budget reconciliation act which Congress passed on December 22, 1987, is a short provision which makes physician charging for office laboratory work a prohibited transaction. It's not so prohibited as selling cocaine, but if a doctor performs laboratory work on a "Medicare eligible person" (i.e. anyone over age 65), he is forbidden to charge the patient for the service. Ay reimbursement must be sought by filing a Medicare claim form, accepting assignment, and hence accepting Medicare's increasingly stingy fee schedule.
Aside from this law's dubious constitutionality, it creates a monstrous administrative headache for doctors. For that matter, it creates a big problem for Medicare's fiscal intermediaries, too. The Prudential Life Insurance Company has just announced it is withdrawing as Medicare intermediary for New Jersey, North Carolina, and Georgia as of next January first. The laboratory billing requirements potentially cause a huge increase in claims volume and a parallel increase in complaints and confusion for the intermediary.
For their part, care physicians face four underlying choices of billing procedure in complying with the new requirements. They might yield to the obvious motive underlying the congressional action, and accept assignment for all service, laboratory and otherwise. That response might simplify bookkeeping, but it could reduce gross Medicare income by an average of 30% (the current average difference between doctors' charges and Medicare "allowable" cost.). Since there would be no parallel decline in overhead, the proportionate loss of net income would be even greater. The second type of approach would be to submit a separate claim form for the laboratory work, or two claim forms (one for laboratory work and the other for other professional services), or write in a "mixed" assignment acceptance in box #25 on the claim form.
All of these claims submission modifications, however, create the same subsequent bookkeeping dilemma: how can doctors credit payments for these laboratory services on their books, when they aren't allowed to bill for them? If doctors do credit the assigned payment to their patient's accounts for something which was never charged to the accounts, the ultimate result is a negative balance or an unintended reduction of charges for whatever else the patient owes. If doctors charge the accounts to balance the books, they are violating the law.
There seems to be no way out of this bookkeeping nightmare except by creating extra bookkeeping accounts to handle Medicare laboratory charges. For those doctors who utilize a computer for their business affairs, it is practical to have the machine create a separate laboratory account for each Medicare patient. For those doctors who still use a manual bookkeeping system, it may be more manageable to create one gigantic account from which Medicare is billed for office lab services, and to which the payments are credited. The underlying accounting theory of this approach is that the patients who are old enough to be eligible for Medicare are officially no longer responsible for office laboratory charges and that the US Government is responsible. That's a bizarre accounting theory, but then it's a bizarre congressional action.
Regardless of extra cost for doctor and Medicare alike, the new law offers doctors no choice but to open separate new bookkeeping accounts for Medicare laboratory services.
For Doctors, Computer Hardware Catches up. Major revisions of Medicare rules have become so frequent that computer software for doctor's offices can be modified quickly enough, only if written in "high-level" programming languages such as interpretive BASIC. Unfortunately, such quickly modifiable code makes inefficient use of the machine; it is "slow".
However, recent advances in cheap computer hardware chips have so greatly accelerated desktop computers that software inefficiency scarcely matters. With "386" processors, doctor's office software written "quick and dirty" in a high-level language can be quickly and cheaply modified to accommodate abrupt changes in HCFA policy. The fiscal intermediaries, on the other hand, must still invest huge resources in painfully reprogramming their mainframe computers in low-level languages.
Paying in Advance is Cheaper
This chapter can be summarized: it's expensive to pay for things on credit, less costly to pay as you go. But payment in advance is cheapest by far. Fully funded prepayment offers a way to make medical care appreciably cheaper for the consumer without reducing services, charges or fees one bit. No rationing, no corner-cutting. Buy exactly as much, get it cheaper.
To understand what the magic is all about, just review some principles of compound interest which are both agreeable to hear and easy to prove. With some possibly exaggerated examples as beacons, the reader is asked to skip through a short description of the environment of complexity which potentially smothers serious proposals to pay a major share of health costs with internal investment income. A healthy distrust of pat answers is quite appropriate; the simplicity of concept does not assure ease of execution. However, since this is not a textbook for insurance executives, the reading public really only needs to extract a slogan: pre-funded health insurance is cheaper, makes medical care cheaper to buy. Have you got that? Cheaper.
Because unfunded health insurance is so traditional we all have a habit of thinking and saying that health costs to the public and receipts by health providers are the same thing. You obviously get the same total whether you add up everything the country spends on health or total up everything the health industry receives. It would seem equally certain that premiums collected by a solvent health insurance company must always, at a minimum, total up to the company's expenses.
However, that's not quite so. If your hypothetical company receives all its premiums in a lump at the beginning of the year, the company only spends the money gradually over the course of the year to reach zero balance on December 31. Since the company only uses one-twelfth of the money each month, it would put the rest into some form of liquid investment which might pay 8%interest in 1988. The whole melting lump would, therefore, generate a 4% return for the year. Consequently, $1000 in premium would buy $1040 in medical care; or, another way to look at it, $1000 of care could be bought for $960. To jump to the end of the argument, $1000 of care might be bought for $100 if prepaid thirty years in advance. Indeed, if prepaid sixty years in advance it could be bought for $9.62. That's the simple principle in the argument that pre-funded health insurance is potentially much cheaper than pay-as-you-go insurance, leading to the rather plausible proposal that we try to find a way to adopt the pre-funded approach. Mind you, there are lots of nits to pick. The rest of this chapter threads through the forest of insurance obscurities related to this idea. However, when saving of 1% translates into five billion dollars a year in the health field, most people would be willing to accept the contention that no amount of nitpicking will defeat the suspicion that pre-funded health insurance could be lots cheaper than our current "pay-as-you-go" approach.
To brush in another argument with broad strokes, it is fortuitous but ideal that heaviest medical care costs happen to be concentrated toward the end of life. If the appreciable medical cost of being born is considered to be the baby's own expense you can a curve of life medical costs which are J-shaped, heavy at the beginning, quite moderate for the next fifty years, then steeply rising. It is more realistic of course to attribute the cost of obstetrics and pediatrics to the young parents, so the most meaning curve is more U-shaped. In fact, a useful graph only begins with the onset of the earning period at about age twenty, has a twenty-year dip in the middle, then rises again. The vital point is there is a calm period in the middle, then rises again. The vital point is there is a calm period in the middle of the storm, just about where the baby boomers find themselves in 1988. If they pre-fund their health insurance, the boomers can have health care pretty cheaply when they need a lot of it. But if savings get dissipated on ski trips and divorces, that generation will have a dickens of time affording a twenty-year vacation after they retire. Provision for retirement is what will ultimately suffer since our whole social structure is organized around the imperative that access to quality health care is a right. If maybe you disagree with Oscar Ewing's 1950 social priorities it will make little difference, because our system of healthcare insurance is currently organized to make certain the vast majority of Americans can spend a lot of money on their health. My yuppie children assure me it is impossible to persuade their contemporaries to set aside investment money in their thirties to provide for a comfortable retirement. But that seems too grim a view of human nature because during the Great Depression era economists were at wit's end trying to get my parent's generation to stop saving so much money and spend a little. The current economic distortion is not either based on some flaw in human nature, it is a fad. The madness of crowds never lasts long.
A fortuitous parallel quirk of the American health insurance system is that very few policies vary the premium with the age of the subscriber, even though average claim cost obviously follows the U-shaped curve. Particularly in direct-pay policies (i.e. no employer in the middle), premiums are usually level across age groups, and the public is universally accustomed to this averaging of costs. If the yup generation started to demand some portion of their own health costs in late middle age, it is hard to see how the presently subsidized older generation would have many complaints, since relatively few of them had been direct-pay subscribers when they were younger. If you tried to switch to a pre-funded system, some gradual transition could probably be worked out by gradually increasing the share of excess premium which goes to permanent funding instead of subsidy for older subscribers. Balancing the basically political question of moral obligation to an older generation which loses its subsidy, there is an opposite political point helping the younger generation to compromise. The yuppie age group is accustomed to relatively high premiums, and might not rebel at continued high premiums which subsidized their own elderly costs rather than the health costs of their parents' generation.
We might now begin a fly-over of the obstacle course by noting that current insurance practice mostly does not even capture short-term interest on the premium "float". Instead of following our hypothetical example of paying the premium at the beginning of the year and reducing cost by 4%, most corporation benefit offices pay their premiums in monthly installments and thus retain most of the interest for their own use. To go a step further, about half of all employer health benefit is self-insured, which is to say the company pays as claims are submitted and therefore allows no interest generation at all. Whatever interest is generated is mostly at the expense of hospitals and doctors, through intentionally slowing down the payment stream, earning interest at the expense of creditors. The fourth section of this book ("Tangles") examines how this short horizon chiseling actually increases the cost of medical care quite a bit.
Furthermore, as mentioned earlier most state insurance commissioners are hostile to the internal accumulation of reserves in the health insurance industry. To understand what is at work here, it is necessary to know about The Premium Cycle. For reasons presently relevant, all competitive insurance goes through cycles in which premiums are unjustifiably low during lean years followed by fat years in which premiums are too high, subsequently followed by more lean years bordering on bankruptcy. Success in the commercial insurance world (outside of health insurance) mostly depends on being so well capitalized that the company can ride out the bad years and make enough profit in the fat ones to average out the cycle. 1987-88 happened to be lean years for the health insurance industry when it was a weekly experience to read of bankrupt HMO's or forced mergers of Blue plan or withdrawals by insurers from the PPO market. it is therefore almost certain we will soon be shocked to read of horrifying increases in premiums which are proposed by frantic insurance companies, and these shocking increases will be opposed by our hero the Insurance commissioner, friends of the people. Well, it's just the insurance cycle, folks. Reflecting the fact that reserves were not permitted to rise to an adequate level during the preceding fat years, the health insurance industry lives on the edge of oblivion, six years out of eight. The health insurance system is recognized to be unfounded; the unadmitted fact is that it is also under-reserved.
By trumping the misleading and largely untrue idea that the money being spent on employee health benefits is money which belongs to the employers, those employers have embraced a heavy trust obligation. If the health insurance company which the employer hires to administer health claims is under-reserved, surely it is essential that the employer maintains reserves at least to protect against the premium cycle. The argument would be that if they kidnap the interest float, employers then necessarily acquire the obligation to fund the reserves. In fact, employers would not dare to do so even if they perceived the duty. Since the tax laws do not permit them to carry benefit money from one year to the next, they may not sequester such reserves in an untouchable fund. However, to maintain large cash balances in the undesignated corporate treasury is a certain way to invite a corporate raider to start a greenmail operation or an unfriendly take-over. Or, in what amounts to the same thing, it tempts corporate management to raid the company in a leveraged buyout.
Health insurance money could finance other corporate raids, too. Health insurance companies are not a particularly profitable business, and most insurance conglomerates only provide health insurance as a service to customers who buy more profitable products. In the current dip in the insurance cycle, the insurance conglomerates have started to learn the old business lesson that "maintaining a full line of products" is almost always a management blunder. On the other hand, a barely-profitable health insurance company handles huge amounts of cash. If its owner happens to be in the greenmail, or arbitrage, or merger and acquisition business, it can be very handy to own a business which can produce millions of dollars on demand for thirty days. It's better than owning a bank since banks are not allowed to supply cash to their owners.
As soon as an investment gets much past one year, it becomes important to focus on "real" interest investment income. Another jargon phrase would be "net, net", which is net after inflation, net after taxes. For example, 15% interest paid during a 12% national inflation produces only 2% real income. If the income tax of 33% is then paid, only a 2% return that you could spend is left the net, net. Indeed, you had better watch yourself, become if taxed 33% of your 15% income, you may only have a 10% net return which inflation then reduces y 12%. You lost 2% that year.
True enough, but the country begins to fall apart when negative returns are more than temporary occurrences. The historical experience for this century is one of real interest returns averaging about 3%, while conservative long-term investing in stock market equities has yielded an 8% return. No one can predict the future, but these historical real interest rates are used as future assumptions throughout this book. The example given earlier should then be recast to propose that $1000 of medical care would cost $xxxx if prefunded thirty years in advance, or $xxxxx if prefunded sixty years ahead. 8% return is only plausible if the risk of investment in equities is built into the assumption. If these comments effectively deal with concerns about unpredictable interest rates and potential inflation, there remains a concern about technological medical inflation which will be addressed in a later chapter.
Meanwhile, the insurance field with singularities of tax treatment. Health insurance provided by employers uses before-tax money. If you earn ten dollars you might ordinarily have only seven dollars left to spend after taxes, but if its put into employer health insurance, you can spend all ten dollars. If that same process were permitted to occur with pre-funded health insurance, the real interest rate would be a third higher than applies to private after-tax investing. Furthermore, ever since the present income tax was imposed in 1913 Congress has made special provision to allow internally generated investment income to compound within life insurance, untaxed.
It now seems time to stop this digression into insurance minutiae and repeat the message worth carrying away from it: if we could find a feasible way to pre-fund health insurance, we would make health care much easier to afford. There is a second message too, which is at least as important. If we could create a trillion dollar investment fund where none now exists, the invigorating effect on the national economy would be astounding. After all, if someone pays 8% to borrow money he can only keep it up so long as he makes at least 12% in. whatever business he then creates with it. Cheer up, congressmen; he will pay half of the difference back to the Treasury as income tax. And he can only function if his employees pay still more income tax as a result of something else which would be created. Jobs.
Dinner at San Simeon in the Old Days
"Joe, I don't want to offend, but I can't help wondering how, how in the world you got to know Joseph Kennedy? It seems so unlikely that a Philadelphia Quaker would ever run in the same circle with such a notorious swashbuckler. How did you meet him?"
The question was pondered, and then agreement nodded. Quakers don't hold with guilt by association, don't fear to be seen in anyone's company, for a purpose. There is that of God, they say, in any man. But my friend's serious nod acknowledged the matter might be thought by some to be strange. "Well, you know I spent much of my time dealing with bankruptcies and receiverships. During the Depression, there was quite a lot of need for that work. One day, the Chemical Bank called me up and said they had come into the problem of Universal Picture Studios out in Hollywood. They asked me to draw up a plan of reorganization for them, as a consultant. I agreed to do so, but it worked out that the stockholders didn't get much out of it. That's very often the case, I'm afraid."
"The Chemical Bank eventually called me up and said they were going to get a heavy hitter in to sell the plan to the stockholders because some were rebelling at the terms. Chemical was kind enough to say it was an excellent reorganization plan, but it just wasn't getting agreement."
"So that's how I found myself in New York when they brought in Joe Kennedy, who listened quickly to me general plan, and they wanted to know just who was the main problem. William Randolph Hearst was mainly it, because of his association with Miriam Davies the movie star. So he told me to get my hat and coat, we were immediately going out to San Simeon, which is certainly a beautiful place.
Sitting at the table at the League, my only possible contribution to this sort of conversation was that I had once paid fifty cents to walk through San Simeon, which is certainly a beautiful place.
"Well, then, you know that dining room with the enormous fireplace, and a big oaken table with a dog crawling around under it. I suppose that's still there. We sat down to dinner with Miriam Hopkins seated at the end, playing hostess, and on her right side, there was Joe Kennedy, the guest of honor. I was seated down below the salt somewhere and watched them all get drunk. There was an awful lot of noise and hubbub, and everybody just seemed to be having a wonderful time."
"Suddenly, Kennedy jumped up, knocked his chair over backward, and shouted out, "Goddam Dog!". Everybody shut up for a minute, but he got his chair back up and sat down. In a few minutes, it was as noisy as ever. The whole thing was ignored, whatever it was."
"Except by me. Coming home on the train when we were alone, I said, Mr. Kennedy, just what was that business about the dog?' "Well,' sez he, 'that women ran her hand up my thigh, so naturally I grabbed her back. And then the goddamned dog bit me!"
I have since reflected on this story and it somehow seems to me Joe Kennedy later bought the studio himself, although maybe I am wrong. It would certainly have been cheap enough. And he later got involved with some other actresses, although perhaps this wasn't his first introduction to the world of glitter since how else would he have been able to invite himself to dinner at San Simeon on the spur of the moment?
Or maybe there is another end to the story, conveyed to me through the medical grapevine. It was that after Kennedy had his eventually fatal stroke, he spent two years constantly repeating a single word. The word "No".
Help for the Failing Business
"Waitress, would you mind bringing my guest some more corn muffins?"
We were back in the Union League, my old friend and I, and just about the last people in the dining room at lunchtime, as we usually were. The members of the League throng into the club for lunch, often a thousand of them at peak times, but the stroke of two o'clock empties out the place as if a silent alarm had rung. It was unthinkable for the waitresses to show any annoyance about members who stayed past the magic moment, and indeed I have occasionally stayed three or four hours with a guest who had important business to transact over the table. Somehow, the all-seeing head waiter gives the necessary whispered orders, and the "help" just melts away. It is, of course, inevitable that the help will grumble about staying past the usual time, but never so the member can hear it. To have to go back four times for special orders of corn muffins, was another thing which must upset them a little, but it was not permitted to show. Anyway, the wizened little old man who was a guest of a member might well have been somebody Real Important. His unfailingly courteous manner apparently led to the assessment that he was "cute".
"You know, George, it is a great pleasure to have lunch with you in public. So many of my friends are afraid to be seen with me, for fear it means their business is in trouble."
"Well, you see, for a number of years I have sort of made a profession, you might say, of helping failing businesses. I guess it's because I hate social work."
"Good Heavens, what's the matter with social work? I have social workers in my family, and the Haddonfield meeting seems filled with social work."
He smiled broadly and nodded pleasantly, but I had to wait for an explanation until a corn muffin was painstakingly buttered a thoroughly chewed. "Well, you see, I think it is much better to take a business with thirty or forty employees and save it from bankruptcy. That way, you don't have to have social work, and you don't have to invent useless jobs for them to do. A business can only be successful if its employees are doing something that people are, you know, willing to pay for. Well, anyway."
Experience had taught me that "Well, anyway" was his signal that maybe we were talking about a subject which ought to be dropped, but which he would continue if I persisted, and I usually did. But forewarned. Warned that although he didn't want to have a flight about it, he held strong views which he wasn't going to abandon. Prolonged chewing of a muffin served as the same kind of signal, I suppose, but muffins were almost too important to be used as conversational props.
As the conversation went on, it turned out he had been involved in the failures and near-bankruptcies of milk businesses, airlines, housing developments in Pittsburgh, a movie studio, lots of very interesting things. Maybe the most interesting was a string of funeral parlors in Brooklyn. Funeral parlors in Brooklyn? How does a Philadelphia Quaker help them?
Although the movements were completely silent, his shoulders shook and he looked for all the world as if he were gleefully saying "Hee, Hee, Hee!" And he then related how he had automated the embalming process by establishing one central factory to embalm the customers. The undertakers would ship the corpses from their sales offices to the central facility, and then return the completed products to their displays rooms. Greatly improved the efficiency, cut costs nicely, and lots of otherwise threatened undertakers were able to continue to provide a livelihood for their families. It was certainly ingenious, and I suppose it was better than social work. At least, it appeared to have been fun, and social work is never fun. Indeed, letting all the social workers I have known run through my mind, I couldn't offhand think of one who had any fun on the job.
"So you are a business doctor?" I was immediately sorry I asked because to answer, "Yes, I guess you could call it that", he had to finish chewing the corn muffin and hastily swallow it. It was the last one, and the waitress was nowhere to be seen.
I was also sorry I said it because I knew his father, mother, brother, daughter, and cousin were all physicians. On the wall of the Pennsylvania Hospital where brass nameplates have been transferred from the rooms of interns after completed training, there are at least six Nicholson names, probably another ten names of relatives by marriage. The very first name is that of Jacob Ehrenzeller, who was the first intern in an American hospital, 1773, and must have been present when the British used the hospital for barracks during our "insurrection". With so many distinguished physicians in the family, Joe's failure to go into medicine might well be a sensitive point, who knows. Rather ungraceful of me to make allusion to a business doctor. As I remember, the mild quip was indeed followed by several minutes of silence.
"Well, Joe as you know I'm very interested in the economics of hospitals, and someday I'd like to see if you have any ideas about how we could make those damned places any cheaper to run. Right now, they are making so much money they don't welcome ideas from strangers, but I suspect their time is coming. Any thoughts?"
He nodded, considered the matter seriously for a moment, and then backed off by remarking that you have to get inside the place and learn every aspect of the business before you can venture an opinion. A courteous and considerate man knew that you offended people by telling them how to run their business. It was insulting to walk into a stranger's world, and before taking off your hat tell him that the solution to his impending bankruptcy childishly did that with their patients, but the patients don't warm to it either.
"Well, tell me. Are there some general principles that are usually of value in approaching a new problem business?"
"Ah, certainly," was the immediate response. "The first thing you do is fire the purchasing agents are crooked. They should be replaced once a year." I gulped. That sort of uncharitable generality was not like him.
"And then," he raced on, "You replace the auditing firm. The outside auditor is only concerned with one thing, which is being invited back by management to do the audit next year. He doesn't want to make waves. He wants to send his trainees to do the work, and so he doesn't like to go to a new business; repeat visits to old friends are the thing. Since it is the auditor's job to tell the owners or trustees about the mistakes that management has made, it is in management's interest to have a comfortable relationship. So, the owners are the last to know what's going on."
For a man whose normal speech was excruciatingly slow and careful, he was roaring into overdrive. "And next, you go after the receivable. Most businesses are too slow and careless in collecting their bills. But if you don't collect your money quickly you never get it. Many businesses have huge amounts of money which they call "accounts receivable" but as a matter of fact they are often nothing at all."
"And then, you get rid your losers. There is no slogan in business more pernicious than the idea of the running of "full service" business, or a full line of products. Inevitably that means your profitable products have to subsidize a whole raft of unprofitable one which is just there to seem complete. If people aren't willing to pay the price you have to charge for something, they are telling you to stop selling it. Meanwhile, you have to jack up the price of your profitable products to pay for this nonsense, and so a full line of products eventually becomes a full line of unemployment."
All of this was pretty exciting, and the ring of intense conviction from a man of experience was convincing, indeed. But, as usual, I had stayed too long at lunch with him, and I simply had to go. Where he was going after lunch was unknown to me, but it was a new idea that people wouldn't want to have him be seen going in their door.
Robert J. Reinecke 10/11/18 10:53 pm
There was a hidden side to Bob. He had first run a jewelry shop in Kansas, where he incorporated a drug store. After a time, he went to Optometry School in Chicago, earning his way running a parking garage. He became highly dissatisfied with Optometry and went to Medical School, then took an Opthalmology residency, where he earned his tuition by testifying in court about shady practices of optometry. One of his most famous private pronouncements was that it required more skill to be a watchmaker than an optometrist.
When he was elected President of the American College of Ophthalmology, seven thousand colleagues were in attendance. The former parking attendant left his considerable estate to the University of Kansas.
Although he was an expert trout fisherman (he sometimes caught and returned to the river fifty trout in a day), he spent most of his spare time running. No doubt the specter haunted him that most of his family died young of arteriosclerosis, that for many years nothing could be done about it except exercise, he got to enjoy running. He often ran five miles every morning and twenty-five miles on weekends. I never heard of him winning the Boston marathon, but he ran almost every year and mostly finished toward the head of the line. He was a skilled home carpenter, a pretty good pianist. He was an early adherent of the computer, and it was there he developed professional fame. Specializing in childhood cross-eyedness, naturally, he understood that the several external muscles of the two eyes had to be finely coordinated. As the muscles on one side of the eye contracted, the muscles on the other eye had to relax. It seemed like a perfect situation for the use of computers, although no one could use it for that without an extensive understanding of how it worked. It required extensive coordination of the computer and its operator, and the work had to be done in very close quarters. It also required elaborate coordination of the operator, the computer and its subject. When he died, he still had no partner, and any successor would have to train himself. Philadelphia had quickly become the center of referral for such cases, and after he died, the young surgeons had to train themselves.
24 Blogs
My Years at Stockley
New blog 2018-08-22 22:39:22 description
The Zimmerman Telegram
Millions died, maybe because of one stolen telegram.
Litchfield to Wilkes Barre, Today
.
Lithuanian Law
 American lawyers teaching law students in Lithuania illustrate the strange contrast between the hunger of some Europeans for American leadership and the rejection of American culture by others.
American lawyers teaching law students in Lithuania illustrate the strange contrast between the hunger of some Europeans for American leadership and the rejection of American culture by others.
Going Down with All Flags Flying
New blog 2018-08-23 19:53:03 description
Looking Beyond Cheap Oil
Working topic: There's plenty of world oil for centuries to come, but cheap oil is mainly found in the Middle East. Even expensive oil would be cheap after a huge investment in transportation, pre-processing and refining. The geopolitical strategy would be to bite this bullet for American consumption while forcing peace on the rest of the world by its continued dependence on the Middle East. The logical outcome of this thinking is to establish permanent Middle East military bases.
Frederick Mason Jones,Jr. 1919-2009
The French horn of the Philadelphia Orchestra, played by the acknowledged premier artist in the history of brass instruments, falls silent.
The Godfather
The chief thug in town turned out to be quite a wit.
Copy of The Godfather 10/11/18 11:09 pm
The chief thug in town turns out to be quite a wit.
COPY of Mary Stuart Blakely Fisher, MD 10/11/18 11:22 pm
First in any class.
The Philadelphia Delegation to he Pennsylvania Medical Society I
New blog 2018-08-27 15:55:05 description
How to Cope with a Trillion Dollars of your own Money.
New blog 2018-09-13 18:00:40 description
Four Prescriptions: Proposals or Reform of Health care Financing Rx. I: PRE-FUNDED HEALTH INSURANCE
New blog 2018-08-30 17:00:36 description
One More Idea, Please
New blog 2018-08-31 16:52:20 description
THREE WAYS TO ACHIEVE FUNDED HEALTH INSURANCE
New blog 2018-09-24 18:36:22 description
Last Year of Life Insurance
New blog 2018-09-18 21:15:00 description
Billing Medicare for Office Lab Work (Without Bookeeping Tangles?)
New blog 2018-09-26 20:50:20 description
Paying in Advance is Cheaper
New blog 2018-09-11 18:00:56 description
Dinner at San Simeon in the Old Days
New blog 2018-10-03 18:01:41 description
Help for the Failing Business
New blog 2018-10-03 19:40:38 description
Robert J. Reinecke 10/11/18 10:53 pm
Born in Kansas where it's windiest, so he hated wind. The answer to his query, where is the least windy part of America? was answered, Albany, New York. Eventually, he was offered the post of Professor of Ophthalmology there, and he happily took it. He bought a house on a trout stream and caught up to fifty trout a day when he wasn't doing computer research on how to correct crossed-eyes in children by lengthening the muscles on one eye while loosening the opposite eye the same amount, a feat that made him famous.
He became a physician in chief at the Wills Eye Hospital, after a stint in the same position as the King's Ophthalmologist in Saudi Arabia. He represented Ophthalmology in the American Medical Association House of Delegates for many years.