The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
It's now moderately complicated to find Perth Amboy, New Jersey, even after you locate it on a map. Like New Castle DE it flourished early because it was on a narrow strip of strategic land, and like New Castle, eventually found itself cut off by a dozen lanes of highways crowded together by geography. It's an easy drive in both cases only if you make the correct turns at a couple of crowded intersections. Both towns were important destinations in the Eighteenth century, but by the Twentieth century, both were pushed aside by traffic rushing to bigger destinations. Industrialization hit the region around Perth Amboy somewhat harder than New Castle, destroying more landmarks, and bringing to an end its brief flurry as a metropolitan beach resort. If you aspire to preserve your Eighteenth-century glory, it's easier if you don't have too much progress in the Nineteenth. In Perth Amboy's defense, it must be noted that Jamestown and Williamsburg, Virginia had just about totally disappeared when noticed by Charles Peterson and John Rockefeller, but neither of those towns was run over by Nineteenth century industrialization. So, while New Castle has treasures to preserve and display, Perth Amboy seems to have only the Governor's mansion like the one notable building to work with. William Franklin, the illegitimate son of Benjamin, was the royal governor installed in this palace shortly before 1776.
Governor's mansion in Perth Amboy
While it is true that some wealthy local inhabitants did a lot to restore and maintain New Castle (and Williamsburg), the Governor's mansion in Perth Amboy was bought and made the home of Mathias Bruen, who is 1820 was thought to be the richest man in America. If Bruen had only had the necessary imagination and generosity, this was probably the best moment for Perth Amboy to have had a historical restoration. Instead, he added some unfortunate features to the mansion; it later became a hotel, and later on, an office building. Public-spirited local citizens are now trying to set things right, but the costs are pretty daunting. Someone has to find an inspired Wall Street billionaire like Ned Johnson to make over an entire town. Occasionally, a state government will do it, as has been done with
Pennsbury. Or a national organization might become inspired, as happened with Mt. Vernon and Arlington. Its present state of peeling paint and makeshift repairs suggests uninterest in Perth Amboy's Governor Mansion by the State, and the absence of whatever it is that occasionally inspires fierce and determined local leadership. Perth Amboy needs some help and needs to forget about its handicaps. Sure, it's hard to commute anywhere, it's even hard to drive across the highways to the countryside. The bluff on the promontory was once quite arresting, now a rusting steel mill occupies that spot. Other than that, it doesn't look ominous or dangerous at all. It's just forgotten.
Pennsbury Mansion
Aside from the Royal Governor's former mansion, it is hard to find a historical marker or monument in this scene of former prosperity and glory, but there is one. Down on the beach is a bronze plaque, commemorating the 150th anniversary of the founding of -- Argentina. So there's a clue, which is not difficult to associate with all of the Hispanic names on the stores, and the Hispanics in evidence on all sides. They all seemed to know that this was once the capital of New Jersey, seemed pleased with it, and could point out the famous building. They are pleasant and friendly enough. Perhaps even a little too comfortable. Because, as William Franklin's famous father once said, all progress begins with discontent.
MINUTES OF THE MEETING OF THE SHAKSPERE SOCIETY OF PHILADELPHIA AT THE FRANKLIN INN CLUB, NOVEMBER 7. 2001:
Dean Wagner in the chair. Other members attending: Ake, Bornemann, Di Stefano, Dobson, Dunn, Fallon, Fisher, Green, Griffin, Madeira, Peck, Pickering, Pope, Simmons, Warden, Wheeler. Guest: J. Goldstein.
The Dean announced the happy news that Messrs. Green, Dunn, and Cramer have volunteered to host the 2002 annual dinner of the Society in honor of the Bard's birthday. We were concerned to hear that Matt Dupee has had to undergo a heart catheterization procedure, but "heartened" to know that all has gone well. An up-to-date directory of the membership is included with these minutes, courtesy of our indefatigable Secretary for Meetings. As we prepared to read after dinner, we welcomed to our midst the current president of the Franklin Inn Club, Jonathan Goldstein.
We began our reading with Act Three, Scene Two of Antony and Cleopatra, and we read through the rest of this long and complex act. The text stimulated one of the most animated evenings of discussion in recent memory, with almost every member present anxious to air his views on one point or another. The Vice Dean stressed the rapid change of scenes and shifting settings of the action. A member recalled hearing in his youth Lord David Cecil's lecture on the play at Oxford, and Cecil's emphasis on the importance of panorama in Antony. In III.ii, we are touched by the painful parting of Octavia from her brother Octavius, who is so cold to all but his sister. Antony and his new bride are off to Greece, but we know where Antony's next travels will take him!
III.iii We are with Cleopatra and her court in Egypt. "Time stopped" while we were in Rome with Antony, commented the Vice Dean: Shakspere continues with the action in Egypt exactly where he left off in the last Egyptian scene in Act Two. The messenger from Rome, whom she beat earlier for unwelcome news, now carefully tells her what she wants to hear: Octavia is short, has a low forehead, is dull in speech, and worst/best of all, she is thirty!
III.iv--- Antony is furious at Octavius for insults to him and loudly tells his new wife that he must defend his honor. Poor Octavia speaks eloquently of her divided loyalties, and of the terrible bloodshed that will follow if Antony does not restrain himself: "Wars ' twixt you twain would be/As if the world should cleave, and that slain men/ Should solder up the rift." She goes to seek her brother and to try to mend the quarrel; Antony has travel plans of his own the minute his new wife has turned the corner. A member commented on the interesting contrast of Octavia, full of moral integrity, to the scheming and selfish Cleopatra.
III.vi---Octavia pleads with her brother to make up the quarrel with her husband, but Octavius is as bitter against Antony as the latter is against him. He tells his naively unbelieving sister that her husband "gives his potent regiment to a troll." Octavius has had Lepidus liquidated, and has seized his possessions; the Vice Dean pointed out that Octavius made no effort to justify this gangland hit against a weaker rival for power. Octavius is "all business, a prig" so we are more sympathetic to Antony than we would otherwise be, despite his petulance and his adolescent emotional impetuosity. Antony has won big battles and has the respect of his veterans; Octavius, his rival, wins no hearts. But Antony is tied to Cleopatra, who to Romans is the very incarnation of moral decadence.
III.vii---Antony makes an irrational, unexplained decision to fight on sea, not on land, where he is the legendary world champion, against Octavius at Actium. Enobarbus eloquently protests, to no avail. Shakspere implies, without explicit statement, that Antony follows Cleopatra' swill in this disastrous decision. He then flees the battle when she does, leaving the field for his rival. Is Cleopatra testing Antony's love? Is she protecting the Egyptian fleet? Is she only interested in protecting Egypt's interests, irrespective of Antony's fate? The Vice Dean commented on the notable contrast between Cleopatra and Elizabeth's brave eloquence addressing her troops when the Spanish threatened invasion when the Armada sailed in 1588. As to Cleo's influence over Antony, a member commented on the parallel to Lady Macbeth's disastrous influence on Macbeth in the play that the Bard probably wrote just before Antony.
III.x---Antony sails after the fleeing Cleo. The Roman Scarus comments that "Experience, manhood, honor, ne' er before/ Did so violate itself." Roman commanders plan to kneel to Octavius. Enobarbus stays with Antony, though reason argues against him.
III.xi---Antony, bitterly ashamed, asks his commanders to divide his gold and be gone to safety. Cleopatra enters to him; Antony condemns her influence over him while acknowledging how completely she commands him. But once she has asked pardon, he is wholly in love again: "Fall, not a tear, I say, one of them rates/ All that is won and lost."
III.xii---Antony in humiliation must send a mere schoolmaster to bargain with Octavius. Octavius will not listen to Antony's requests to retire to Greece to private life, but Cleopatra will be protected if she kills or hands over Antony to his rival.
III.xiii---Thidius, sent by Octavius to Cleopatra, is found kissing her hand by Antony, who has him whipped a shocking offense to Octavius. Antony challenges Octavius to a duel to settle their quarrel, provoking satiric scorn from Enobarbus. But Enobarbus struggles to justify staying true to Antony. As Cleopatra flatters Octavius' agent, Enobarbus declares that he must "find some way to leave" Antony. Cleopatra finds wonderful language to claim Antony's love once again. Antony, swinging from despair to jubilation, calls, "Come,/ Let's have one other gaudy night: call to us/ All my sad captains, fill our bowls once more." But Enobarbus hears only the voice of irrational infatuation, and declares, "I will find some way to leave him."
OUR NEXT MEETING WILL BE ON NOVEMBER 28. WE WILL BEGIN OUR READING AT ACT FOUR, SCENE ONE
Respectfully submitted Robert G. Peck Secretary for Minutes
WITH British troops in the process of disembarking at New Brunswick, apparently intent on hanging rebels, Robert Morris and John Dickinson annoyed everybody by refusing to sign the Declaration of Independence. Both were fully engaged in the Revolution after the fighting finally got started, and Morris signed up in August 1776. Dickinson had some further reasons of his own, but Morris explained his position quite succinctly. He didn't mind being a British subject, he didn't want a new King, what he wanted was Constitutional Liberty. There is no record of his being directly confronted about this later, and thus no detailed explanation. But whatever did he mean?
Iliad and the Odyssey
Morris was of course very bright, even brilliant as a businessman. He had an astonishing memory for detail and was capable of holding his own counsel. He was a person of great daring and prodigious amounts of work. But there is very little evidence that he thought it was useful to be mysterious, or deep. So why not take him at his word, which was essentially that what mattered in a government was whether it kept its promises and allowed its citizens all possible Liberty. It did not matter whether the government had a king, or seldom mattered much who that king was. What mattered was whether it kept its promises, and for that a Constitution is useful. There is no great pleasure in being capricious and arbitrary, so a king who leaves the citizens alone is mostly the best you can ask for. It does, however, help considerably if the rules are fair, clear, and binding. Beyond that, it is unwise to go about toppling governments in the vain hope that a new one is somehow better than the old one. This is putting words into his mouth, to be sure. What he did say was he saw no advantage to getting a new government when what we wanted was Constitutional Liberty. Eleven years later, he was a personal friend of just about everyone with the power to design a new government. Washington lived in his house, or in one next door. Ben Franklin was a business partner. Gouverneur Morris was his lawyer and partner. Just about everybody else who mattered was meeting with him in secrecy for months at a time, in the Pennsylvania Statehouse. And so on.
An essential part of this puzzle of Morris' role could be that the American Constitution was very close to unique in being written out as a document, like a commercial contract. The British Constitution was unwritten at the time and continues to be unwritten today. Many other members of the British Commonwealth operate without a written constitution. And in fact, what passed as constitutions for thousands of years have been unwritten; it was the written American one which was the novelty, not the other way around. It may stretch matters a little to describe the Iliad and the Odyssey as constitutions, but they do in fact describe the system of governance of the Ancient Greeks, clarifying many axioms of their culture for which they were willing to fight and die. We are able to understand the rules for Greeks to live by from reading Homer, almost surely better than we understand the rules of American culture by reading The Federalist Papers. Modern students of geometry, for another example, are taught that all the rules of Euclidian geometry are based on a few axioms stated at its beginning. Change one of those axioms, and you make mathematics unrecognizable. Even Newton's Principia are now seen by mathematicians to be rules which apply only to our universe for certain. There may exist many other universes to which they do not apply. Axioms are themselves mostly regarded as unprovable assumptions. A Constitution, therefore, is regarded in modern times to be much the same thing as a set of mathematical axioms. With one new exception: they are written out on a piece of paper for all to see and agree to -- just like a commercial contract. It would not be surprising to discover that America's great merchant trader, Robert Morris, was horrified at the idea of depending on Vestal Virgins or Judges, or Kings, for their recollection of what the contract says. It, therefore, seems quite natural for a maritime merchant to be agitated by having the rules of British society depend on what King George III chose to emphasize or ignore. Write it down, negotiate it, then tell us what you want so we can agree to it; that's a proper way to define Constitutional Liberty and limit disputes. International maritime trade could not be conducted in any other way, because sea captains who feel abused in a foreign port can abruptly up-anchor and sail away, never to return to that port again until or unless local rules are clarified.
Unless someone discovers some relevant documents in a trunk in the attic, that's about the best conjecture to be made about the American novelty of a written constitution, and its transformative effect on the legal system of all other nations which have one. It would still be nice to know, for certain, whose idea it was.
Howard Callaway, noted historian, recently held forth at a meeting of the Franklin Inn Club about the Progressive Movement of the early 20th Century. His interesting point was that perhaps William James really started it all. The James brothers, William and Henry, were very rich and spent nearly twenty years in Europe. Their ideas may not have originated in Europe, but they certainly had a European tinge to them. Perhaps it is fair to surmise that the Progressives grew out of reaction to the Gilded Age, around 1870, which Howard feels was the last great episode of globalization before the present one.
In spite of the very European origins of Queen Victoria and her family, the British aristocracy has always feared and distrusted Europe. When Britain discovered it couldn't conquer Europe (or America), it turned its attention to developing a great commercial empire by colonizing Africa and East Asia. That led to building a Navy and establishing naval refueling stations at strategic places around the globe. Meanwhile, the Spanish empire was deteriorating, and colonization took on the form of competition between England, France, and Germany for the remnants of the Spanish empire. For background music, the Dreyfus episode led to or was prompted to lead to, an anti-military attitude that had considerable world-wide effect, essentially none of the above. In time, the none of above military attitude fused with Progressivism of the environmental sort which viewed industrialization as the enemy.
William McKinley
In a sense, American attitudes were influenced by William McKinley, who managed to convince labor they would be better off by advancing the cause of their bosses. Part of the reaction to this was the Populism of William Jennings Bryan and Robert LaFollette. McKinley's assassination and the promotion of Teddy Roosevelt was an unexpected turning point in American politics. Meanwhile, Admiral Dewey's fleet was stationed in Hong Kong. This association between America and Great Britain, along with secret German attempts to intervene in unobtrusive ways during the Spanish-American War were important factors in the later alliance between Britain and America in World War I. The burgeoning alliance between labor and management which McKinley was well along toward making the dominant force in American politics, was thus precipitously switched toward Progressivism by McKinley's assassination, which revealed he had made the one major blunder of selecting Teddy Roosevelt as his vice president, who in turn made the same blunder in reverse by selecting William Howard Taft as his own successor. The splitting of the Republican party between Roosevelt and Taft made possible the election of Woodrow Wilson, the college professor.
It thus can be concluded that the repeated switching between Conservatism and Progressivism during the Presidencies of McKinley through Wilson was the main source of the present rearranged coalitions we call the Republican and Democratic parties. It only remained for Franklin Roosevelt to complete the process by fitting the South, Catholics, and Jews into the Democratic Alliance, and Richard Nixon to undo it partially with switching the South and the Catholics back into the Republican party. The demography of the parties has changed more than the ideology, which tends more toward a coalition of business and Southerners versus blue-stocking progressives linked with labor union populists. Underlying all of this is the general acknowledgment of the need for a two-party system. Instead of having five or six small parties, the ultimate choice is whether a dissatisfied sub party is disaffected enough to switch parties. The nation is geographically so large and the subgroups so scattered that almost everyone except recent immigrants instinctively respects the two-party imperative.
It was expedient to leave certain phrases in the Constitution intentionally vague, but the overall design is clear enough. Just as twenty-eight sovereign European nations now struggle to form a European Union, thirteen formerly sovereign American colonies once struggled to unify for the stronger defense at a reduced cost. Intentionally or not, that created a new and unique culture, reliant on the constant shifting of power among friendly rivals. Everybody was a recent frontiersman, trusting, but suspicious. It still takes newcomers a while to get used to it.
So the primary reason for uniting thirteen colonies was for a stronger defense. As even the three Quaker colonies of New Jersey, Pennsylvania and Delaware could see, if you are strong, others will leave you alone. In time, the unification of many inconsequential behaviors created a common culture of important ones; and in time that common culture strengthened defense. At first, it seemingly made little practical difference locally whether construction standards, legal standards, language and education standards and the like were unified or not. Except, that in the aggregate, it forged a common culture.
The practice of Medicine was certainly one of those occupations where it mattered very little whether we were a unified nation. Unification of medical care offered a few benefits, but mostly it didn't matter much, right up to 1920 or so. Even then I would offer the opinion, that unification of the several states (with consequent Free Trade) only made a big difference to health insurance, and still made little difference to the rest of medical care. In fact, there are still about fifteen states with too little population density to provide comfortable actuarial soundness for health insurance, as can readily be observed in the political behavior of their U.S. Senators. Although the number of low-population states gets smaller as the population grows, there are even so perhaps only ten big states where multiple health insurance companies can effectively compete within a single state border. Quite naturally the big-state insurers expect one day to eat up the small ones. By contrast, the nation as a whole, the gigantic population entity which Obamacare seeks to address, has far too many people spread out over far too large an area, to be confident we could unify them into one single program. Dividing the country into six or seven regions would be a much safer bet. That's the real message of the failure of the Computerized Insurance Exchanges -- far too much volume. And the coming failure of the Computerized Medical Record -- with too much complexity. With unlimited money, it can be done, because diseases are disappearing and computers are improving. But why struggle so hard?
It is at least fifteen years too early, and mostly serves the interest of insurance companies, if they can survive the experience. At the same time, we are at least fifteen years away from growing the smallest states to the point where we could decentralize. It's really a situation very similar to the one John Dickinson identified, James Madison briefly acknowledged, and where Benjamin Franklin improvised a solution. In their case, it was a bicameral legislature. In the case of medical care, it could be an administrative division of revenue from the expenditure. It could be the cure of a half-dozen chronic diseases. It could be six regional Obamacare. But creating one big national insurance company during a severe financial recession is something we will be lucky to survive.
Returning to the Constitutional Convention, an additional feature was added to the tentative 1787 document to respond to protests from small component states. They objected that whatever the big-state motives might be, small states would always be dominated by populous ones with more congressmen if a unicameral Legislature is made up of congressmen elected by the population. Pennsylvania had recently had a bad experience with a unicameral legislature. So a compromise bicameral legislature (with differing electoral composition in the two houses) was added to protect small-state freedoms from big domineering neighbors. Even after the Constitution was agreed to and signed, the states in ratifying it still insisted on a Bill of Rights, especially the Tenth Amendment, elevating certain citizen prerogatives above any form of political infringement, by any kind of a majority. These particular points were "rights"; individuals were even to be insulated from their own local state government. The larger the power of government, the less they trusted it.
John Dickinson of Delaware, the smallest state, soon made the essential point abundantly clear to a startled James Madison, when he pulled him aside in a corridor of Independence Hall, and uttered words to the effect of, "Do you want a Union, or don't you?", speaking on behalf of a coalition of small states. It was probably galling to Dickinson that Madison had never really considered the matter, and went about the Constitutional Convention airing the opinion that, of course, the big states would run things. Dickinson, who had been Governor of two states at once, had observed the effect of this attitude and wasn't going to have more of it.
Delegates
Benjamin Franklin, who for over 40 years had been working on a plan for a union of thirteen colonies (since 1745, long ago producing the first American political cartoon for the Albany Conference), devised the compromise. It was essentially a bicameral legislature -- with undiminished relative power in the Senate for small states. In this backroom negotiation, it was pretty clear Franklin held the support of two powerful but mostly silent big-state delegates, Robert Morris and George Washington. These were the three men of whom it could be said, the Revolution would never have been won without each of them. In 1787 they were still the dominant figures in diplomacy, finance, and the military. All three were deeply committed to a workable Union, each for somewhat different reasons. Now that a workable Union was finally within sight, parochial squabbles about states rights were not going to be allowed to destroy their dream of unity.
And so it comes about, they gave us a Federal government with a few enumerated powers, ruling a collection of state governments with regional power over everything else. And since big-state/small-state squabbles are unending, almost any other solution to some problem repeatedly, seemed preferable to disturbing what holds it all together. On the other hand, the Industrial Revolution was beginning at about the same time, and people who recognized the power of larger markets almost immediately set about attacking state-dominated arrangements, systematically weakening them for a century, and redoubling the attack during the Progressive era at the end of the 19th Century. Attacks on what seemed like an abuse of state power, the power to retain slavery, and later the power to perpetuate white racism, were claimed to justify this attrition of states rights. The ghost of the Civil War hung over all these arguments, restraining those who pushed them too far.
However, the driving force was industrialization, with enlarged businesses pushing back against the confinement of single-state regulation within a market that was larger than that. This restlessness with confining boundaries was in turn driven by railroads and the telegraph, improving communication and enlarging markets, which offered new opportunities to dominate state governments, and when necessary the political power weakens them. One by one, industries found ways to escape state regulation, although the insurance industry was the most resistant, whereas local tradesmen like physicians found it more congenial to side with state and local governments. The 1929 crash and the Franklin Roosevelt New Deal greatly accelerated this dichotomy, as did the two World Wars and the Progressive movement from Teddy Roosevelt to Woodrow Wilson. The Founding Fathers were said to have got what they wanted, which was a continuous tension between two forces, supporting both large and small governments; with neither of them completely winning the battle.
Insurance Monopoly
The medical profession further evolved from a small town trade into a prosperous profession during the 20th century, but the practice of medicine remained comfortably local. Even junior faculty members who move between medical schools quickly come to realize their national attitudes are somewhat out of touch with local realities. For doctors, state licensure and state regulation remained quite adequate, and state-regulated health insurance companies paid generously. State-limited health insurance companies had a somewhat less comfortable time of it, but the ferocity of state-limited insurance lobbying, as exemplified by the McCarran Ferguson Act, perpetuated it. The medical profession watched uneasily as the growth of employer-paid insurance extended the power of large employers over health insurance companies beyond state boundaries, and thus in turn over what had been medical profession's kingdom, the hospitals. And the medical profession also had to watch increasing congeniality with big government extend through businesses, unions and universities, fueled by overhead allowances of federal research grants and finally in 1965, federal health insurance programs. Nobody likes his regulator, but national organizations inevitably prefer a single regulator to fifty different ones. Furthermore, everybody could see that health care suddenly had lots of money, and naturally, everybody wanted some.
There is nothing naturally inter-state about medical care -- except health insurance.
It was all very well to pretend that health care was out-growing local-state regulation, but those on the inside could uneasily watch the federal/state competition for control, with the federal government repeatedly stacking the deck more in its own favor. Aside from federal program interventions, there is still nothing naturally inter-state about medical care -- except health insurance. Doctors, hospitals, and patients all tend to remain local, but insurance can easily cross state lines if regulation permits. Even in insurance, small states have difficulty maintaining actuarial stability, driving health insurance toward one-state monopolies. With a few big-state exceptions, even most health insurance companies prefer single-state monopoly status to federal regulation because it facilitates marketing. To praise the virtues of insurance competition is fine, but if sharing the local market means struggling for adequate risk reserves, nationwide regulation will inevitably lead to domination by a few big-state insurance companies. Small-state insurers would enjoy access to a national market; but blocked from it, they need to retain a local monopoly to survive. Fleeting thought might be given to Constitutional Amendment, but there are probably always going to be enough states which consider themselves small, to block the two-thirds requirement for Amendment. Imposing nationwide uniformity by force would possibly improve standards, but uniformity is increasing rather than decreasing, so the argument is not a strong one.
To be fair about it, there was not a strong case for state regulation, either. It could have been argued that uniformity and reduced administrative costs favored central regulation over-dispersed control, because of improved efficiency; and few would have argued about it. Until the ACA insurance exchanges crashed of their own weight around the ears of hapless creators, that is, unable to do what Amazon seems to do every day, and raising quite a few embarrassing recollections. Recollections of the mess the Sherman Antitrust Act inflicted on local medical charity in Maricopa County, Arizona. Recollections of the "Spruce Goose" airplane that Howard Hughes made so big it couldn't fly. Recollections of the gigantic traffic jam strangling the District of Columbia every weekend. And, reminders that 2500 pages of legislation remain to be converted into 20,000 pages of regulations which it would take a lifetime to understand. Suddenly, let's face it, retaining state regulation of health care, or not rocking the boat, gets a lot better press. It might even work better than the national kind, especially in an environment where no one expected a perfect solution, and just about everyone had heard of the Curse of Bigness. When we first discovered that use of health insurance added 10% to the cost of health care, it had seemed like an easy place to extract 2% of the Gross Domestic Product for better things, just by streamlining administration. But after the health exchange fiasco, some people begin to wonder if 10% is just what it costs to use insurance to pay for healthcare. If that is the case, perhaps we should look at other ways of paying our bills, not just a different regulator. Nobody would pay 10% just to have his bills paid, if he understood what he was doing.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.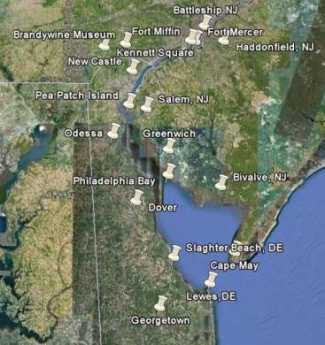 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.