The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
When there is inflation, the value of money goes down, so you might expect interest rates -- the rental cost of money -- to go down, too. However, people anticipate higher prices, so lenders build a premium into the interest rate structure to compensate for the value of the money to be lower when it is repaid. That raises interest rates, and the Federal Reserve will generally raise them even higher to put a stop to inflation. So, buying and selling bonds is a zero-sum game, far riskier than it sounds. Consequently, there is a flight toward common stock, thus raising its price. Meanwhile, inflation usually hurts business, tending to lower the stock prices. As a consequence of all these moving parts, long-term investors are urged to buy at a "fair" price and never sell, no matter what. Even that strategy fails for any given stock because somehow corporations seldom thrive for more than seventy-five years. So, the advice is to diversify into a basket of stocks, and the cheapest way to get that basket is to buy an index fund. In a sense, you can forget about the stock market and let someone else manage the index, for about 7 "basis points", that is, seven-hundredths of a percent. All of this explains the choice suggested for Health Savings Accounts of buying total market index funds. Limiting the universe to American stocks is based on a political hunch that it reduces the chances of harmful Congressional protectionism. Having said that, a Health Savings Account must raise cash from time to time, and to guard against forced selling in a down market, some average amount of U.S. Treasury bonds will have to be maintained. Ideally, the number of Treasuries would be small for young people, and grow as they get older, and therefore more likely to get sick. Pregnancy is the one universal cost risk for younger people, and they know better than anyone what the chances of that would be in their own case.
This approach is greatly strengthened by reference to the modern theory of a "natural" interest rate, to which the whole system has a tendency to revert, if only we knew what the natural rate is. It is not entirely constant, but over time it seems to be something like 2%. If we knew for certain what it was, we could set a goal for perpetuities like the Health Savings Account to be "2% plus inflation". Since inflation is targeted by the Federal Reserve as 2%, that would amount to an investment goal of 4%. If you can buy an American total market index fund consistently gaining at 4.007 % per year, you should buy and hold. If it rains less than that, it is either run by incompetents, or it is a bargain which will eventually revert to 4.007% and pay a bonus. If, on the other hand, it gains more than that, there exists a risk it will revert to the mean. That it is being run by a genius is sales hype to be ignored. We suggest buying into it in twenty yearly installments, which should balance out the ups and downs, so then you can forget about even this issue.
But don't count the same issue twice. In order to assure a 2% real return, it is necessary to obtain 4% in the real world of 2% inflation, and the compounded income of 4% accounts for both in equal measure. A compound income of 6%, however, is two-thirds inflation / one third "real", so artificially raising interest rates to control inflation can progressively overstate the requirement, and hence overdo the deflationary intent. Conversely, when the Federal Reserve fails to raise interest rates as Mr. Greenspan did, the result can be an inflationary bubble. The central flaw in adjusting prevailing rates to current natural rates is that we do not know precisely what the natural rate is. To go a step further for immediate purposes, we are also uncertain how much deviation there is between medical inflation and general inflation. As a result, the best we can expect is to make as much income on the deposits as we safely can, and continuously monitor whether the premium contributions to Health Savings Accounts might need to be adjusted. And the safest way to do that is to have two insurance systems side-by-side, one of them a pay-as-you-go conventional policy for basic needs during the working years, and a second one whose entire purpose is to over-fund the heavy expenses at the end of life and the retirement years, permitting any surpluses to be spent for non-medical purposes. With luck, the beneficiary might retain a choice between increased premiums, and increased (or decreased) benefits.
If these calculations are even approximately close, the financial savings would be several percents of GDP, a windfall so large that mid-course adjustments could be tolerated.
It's only a beginning, but the reader now has a summary of where the Classical Health Savings Account stands, with a few suggested amendments to make it better. Remember, with essentially no changes and with minimal marketing effort, C-HSA has acquired fifteen or so million subscribers. Certain features need to be emphasized before it can extend to the rest of life, and harmless modifications made to accommodate the extensions. At the moment, the appeal is mostly to people between the ages of thirty and fifty, while with a few additions it could extend to everyone who wants it. Beyond that, it stumbled onto some features which would make an excellent foundation for wealth creation, for those who don't believe everyone should just invent something and become a billionaire. But to achieve it we have to get past the idea that everything in the public sector must disappear into a black hole, never to return to private hands. Read on, but handle with care.
FLEXIBILITY: Health Insurance, plus Retirement Income if you survive.
Hidden Advantages, Mostly Unexploited. C-HSA has the flexibility to manage the transition between health insurance and retirement income. Health insurance is the primary need of the past, retirement income the primary need of the future. It's a lucky feature that relatively few people have both problems because very few of us could afford to address both of them. At one time, health care was a major concern of employees; nowadays, it is a major concern of retirees. The day will eventually come when so few get seriously ill, other than terminal care, that we can fund retirees for retirement living, and let them dip into the savings if they occasionally get sick. But that's at least a generation away. At every stage, there must be some who generate a surplus, because otherwise, some will remain impoverished.
The C-HSA lets you judge your own needs as they come up, rationing what you think you need less of, in order to pay for what you suppose is your likely future need. That's the 2015 problem, and it has no good solution except flexibility -- and good luck. Because of the fruits of research, the 2050 problem is going to be retirement income, and it will need a source of revenue. The flexibility of C-HSA allows this choice to be made individually and eventually permits Medicare to be liquidated to finance it. C-HSA scarcely needs any changing to make this adjustment; Medicare is the program which needs to face the future, make itself modular, and provide ways for people to buy their way out of it, in pieces. Until changes are made to invite partial buy-outs, there is little HSA can do except buy out of Medicare entirely. It will be a long time before many people will take such a big step, but much sooner, they will surely see parts of it they would like to drop in favor of -- flexibility.
BOUNDARIES: Any surplus belongs to the subscriber.
Substantial Improvements, Without Disturbing the Basic Structure. Much will depend on the early administration of the Affordable Care Act. If it cannot accommodate the needs of big business in their suspended negotiations, or if it proves to be inordinately expensive, it will collapse. Most of the many Republican candidates for President have endorsed HSA as a substitute policy, and Mrs. Clinton has yet to reveal how she will get out of her HMO proposal of ten years ago. By this time, she surely has learned how distasteful the American public finds HMO when run by non-physicians. In coming chapters, we will describe how essentially the same idea was earlier proposed by physicians, and blocked by the Maricopa Decision of a minority of the United States Supreme Court. Physicians never dreamed anyone would direct a medical organization, except physicians, so there is room for revised opinions; but the twists and turns of politics will eventually dictate where physicians will stand. It is amazing how many people want to run medical care, but how few of them want to go to medical school.
Once we all have basics, we can look around for luxuries.
Benefit Package
The present stance of HSA proposals is that the Affordable Care Act would be improved by substituting Catastrophic health insurance, or else First and Last Years of Life Insurance, for the present hodge-podge collection small mandatory benefits. The alternatives, either the employer-based system or the European single-payer system, similarly become unaffordable when made universal. Universal coverage is indeed desirable, but not to the point of defining that nothing is permitted unless it is universal. If we must have mandatory health insurance, let it cover basics alone --either universal experiences like birth and death or universal fears, like a massive expense. Any degree of choice by politicians or bureaucrats is intolerable, and choice by physicians is barely tolerable. Once we all have basics, we can look around for luxuries. Is that too much to ask?
WEALTH CREATION: Tax Exemption, Compound Interest, then Passive Investing.
Future Dreams
The Golden Surprise. In this book, once we have explored some of the Hidden Economics of Healthcare, we will be ready for the big surprise, which is how much money can be created by changing the insurance design. It might take us a decade to perfect, and several chapters to describe. When lifetime coverage seemed to become possible through the pathway of the tax-exempt Savings Account, supported by Catastrophic fail-safe coverage, we made an amazing discovery. As one of the creators of the idea, I can tell you we had no idea the invested income in these accounts could generate so much money.
That came about by our determinedly avoiding government control and seeking new pathways the government could not follow. It may be a delusion on my part, but I believe the temper of the public will never tolerate government ownership of a private business. Although some far Eastern nations have tried it, their present direction is away from it. Even the Indian subcontinent and the more socialist members of the European Union have found it doesn't work. Very few American college students, however liberal, persist in the notion of government running a business, once they emerge from the campus into the real world. The African and South American dictatorships wallow in failures of the oligarchy approach, even when supported by economies based on natural resource discoveries. Consequently, I believe we will emerge from this and future recessions with the cultural belief that collective government ownership of the means of production, is a bad idea. I believe the wide-spread distribution of common stock will make us stronger capitalists, not weaker ones. That's a hint of what follows.
All of above, and probably more. In all of these areas, the danger of conflict of interest would arise, but somehow it has always been managed. In fact, medical ownership or control of ancillary services has probably declined, although it is likely the medical owners have usually been happy to be rid of the distraction. Medical malpractice insurance is probably an example of medical owners filling an unfilled need. When competition returned to the field, the owners have generally preferred being rid of the unpleasantness, rather than enjoying distasteful profits.
If to all these associated for-profit corporations, is added the educational loan system for healthcare providers, plus the myriad institutions to house the patients, it starts to become clear the danger of monopoly control is a small one. While there is no doubt local monopolies would arise, and some instances would occur of provider control of them, the industries now making up 18% of a gross national product would greatly dwarf the number of providers. Physicians were paid 20% of the healthcare dollar in 1980, but only 8% today, as an example of how great the field has become dominated by non-professionals. The scientific field has become so huge and so attractive in itself, that comparatively few medical professionals of eminence are interested in business careers. It is true professionals lacking eminence are more attracted to such activities, but the resulting peer pressures strongly favor the few eminent professionals who allow themselves to be involved.
A long time ago, a rich oriental man flew five thousand miles to ask me a question, "What is the secret of a long life?" I was so startled by the experience I never did ask him why in the world he would think I knew the answer to such a question. But after a few seconds, I blurted out an answer. "The secret of long life," sez I, " is never get sick." I don't know what his opinion of my profundity was. But I do know what he died of. He was executed by his government, so I hadn't given him the right answer to his question.
At other times, people especially my children, asked me how to get rich. After some practice, I developed a pat answer to that one, too. "The secret of getting rich is to spend less than you earn." What I realized too late to be useful, was that "Don't get sick and don't spend more than you earn", is a peculiarly American viewpoint, a Philadelphia attitude, and ultimately a Quaker one. It probably explains why there have been so few Pennsylvania Presidents of the United States, few Nobel prize winners, and relatively few Philadelphia glitterati in general.
Because, "Avoid risky behavior" comes closer to the right answer, since risky behavior is a fairly good pathway to glitterati success, and the Quakers had figured out it was a fairly good trade-off, to prefer longevity with prosperity. When I worked at the National Institutes of Health, I was struck by how many eminent scientists went through red lights, and otherwise exhibited risky driving behavior. Everybody knows eminent politicians play around with risky sexual behavior, as do movie stars and glitterati in general. But it is less noticed that America has an even larger proportion of risk avoiders who use that method to live long and prosperously. America has developed an environment where it is possible to get old and prosperous without so much tiresome risk-taking. Kingley's famous text of, "Be a good, sweet child, and let who will be clever", doesn't quite get to the root of it. It's the risk you want to minimize, not cleverness.
And the verb is minimizing, not eliminate. The Quaker term is "steely meekness". And a bothersome American response comes from Winston Churchill, "If the enemy comes, be sure to take one with you."
Department of Health and Human Services Bureau of Program Operations
Mr. George R. Fisher III, MD
Pennsylvania Medical Society
20 Erford Road
Lemoyne, Pa. 17043
Dear Dr.Fisher:
The Administrator has asked me to respond to the Pennsylvania Medical Society proposal on the subject of cross-over billing for Medicare and Medicaid. You described a difference in Pennsylvania between Medicare and Medicaid requirements for identification of individual providers who file a claim(s) for service as apart of a group practice.
After examining the problem, I find that the Medicaid statute requires identification of the individual within the group to produce a profile o care and service for each individual provider and to properly account for payments. Consequently, I must continue to require the identification of each individual provider practicing in a group for Medicaid claims.
REgarding Medicare requirements, we are aware of the different requirements of each program and are working to bring the two programs closer together. HCFA staff is preparing background material and analyses for my consideration. I will be addressing these issues in the near future and hope we can resolve these differences to the satisfaction of all parties.
Thank you for sharing your concern.
Sincerely yours,
John C. Berry
Director
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.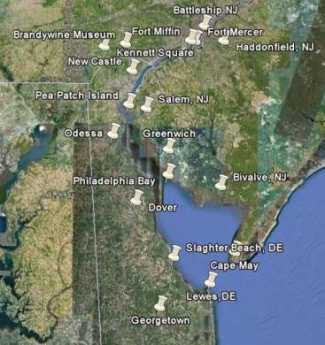 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.