Related Topics
No topics are associated with this blog
Gently Nudging Medicare
That's what the first section of this book was intended to work around, and it might seem prudent to end the debate on that level. Continuing our present system amounts to "muddling through" an impossible situation without offering alternatives that might lead to success. That is, present systems cannot reasonably be expected to pay for a century of health care, let alone the staggering costs of retirement which are a direct consequence of improved longevity. The single-payer proposal might (or might not) reduce health insurance costs somewhat, but it implies a huge health subsidy which would make total costs much worse and makes no provision at all for retirement. In fact, it exposes the short-sightedness of blaming all our problems on insurance: having addressed that with more huge debts, it leaves us up to the total health cost creek (including extended retirement) without even a paddle. The first part of this book shows us a method to address the whole problem, even though present funding might only pay for the healthcare part of it. It's novel contribution is to separate individual savings from shared expenses, and then to use compound interest as an unexploited revenue source. Because there would be a continuing need to make revenue sources more comfortable, the last section of this book explores them. If these later proposals accomplish little more than stirring up better proposals, that's a long step forward from where we now are.
Confusing Costs with Charges. The first graph shows the "costs" we already spend per person for healthcare, adapted from Dale Yamamoto, the actuary who has written most on the subject. You will pardon a brief excursion into jargon. Costs are compared with idealized revenue. Costs are ordinarily more reliable than revenue projections, both of which must eventually total the same final amount, so in real life costs and revenues respond to each other rapidly. In this case, costs are based on reimbursement reports, both overpayments, and underpayments, themselves responding to cost shifting and artifacts of cost-to-charge distortions. Reimbursements are also modified by competitive loss-leaders, mis-projections, and changes over time. They are then further distorted by magical-deluded politicians. (An example of that was the imposed regulatory rule, that inconvenient between-age costs may not exceed a certain ratio to each other). Costs change over time, and they respond with alacrity to reimbursement decisions. We have to take the actuary's word that approximating the deductibles and co-pay costs makes little difference in the final result, but one caution is firm. Since these figures only represent the ingredient cost which providers send to the insurance company, they necessarily omit the cost of health insurance itself. It would be informative to know whether insurance costs add 1% or 20% to the average cost, and then decide for ourselves whether insurance cost makes a significant difference. Since it becomes obvious these curves are all approximations, their apparent precision might be treated with less caution than the selection of other inputs. The shape of the curves is accurate enough, but since we are mainly interested in comparisons between insurance approaches, it is disappointing to find so little data to use.
|
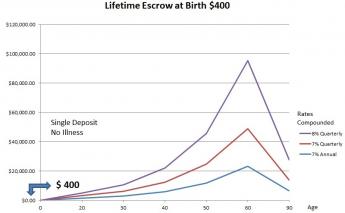
Re-insuring the Last Year of Life Turning now to the above graph as a 13 introduction to a new topic, its revenue projection comes from investing $400, at birth and in escrow (You can't touch it for other things.). Seven percent is easy to calculate in your head since it doubles every decade. Eight percent is what we estimate to be the highest (safe, net, average long-term) return an investor could expect to maintain for decades, also happening to dramatize the major improvement in final income which is possible from very small, but consistent, efficiencies. Stated another way, it illustrates what it costs the HSA depositor not to resist HSA intermediaries who suggest interest-free deposits for long periods of time. Depositors should propose instead to put the money into escrow at long-term rates; this can be one advantage to dealing with a small-town banker in person. By current law, deposits stop at age 65, and the decline in balance to age 85 represents the removal of retirement income. Somebody is going to gather this income, and it might as well be the HSA depositor.
If you put it in escrow so you can't spend it, you become entitled to long-term rates, but if you insist on a demand account, you get demand rates, which right now are quite low. To solve this dilemma, we propose using an escrow to pay for your last year of life, which is a pretty certain long-term bet. That leaves the rest of the account available for routine health costs, and the government should be persuaded that removing up to 30% of their costs is a good deal for them, too.
(While only 50% of total health costs are paid by Medicare, 30% of what Medicare does pay is for the last year of life, which is what we are coming to. It grows to 50% of costs for people over 85 in the last year of life, and improved longevity pushes more people into that group. The sole financial advantage to growing old, is compound income increases considerably at the far end, too. They both follow J-shaped curves. At this distance, it is not entirely certain to know how these two factors to balance.)Actually, we are about to propose that part of the Medicare withholding tax, collected between ages 25-65, be isolated (escrowed) as the source of long-term money deposited in HRSA accounts because the money is collected for Medicare -- whose own total costs would be reduced by expunging the last year of life costs. Because all such innovations have uncertainties, the $400-at-birth illustration is offered to show the way shortfalls could be supplemented at low cost, but if unneeded, used as more retirement income. The purpose of using a single-premium illustration is to anticipate that payroll reduction ends at age 65, while the last year of life occurs twenty years later on average. Another direction to take with a surplus might be to expunge costs for the last two years of life. Or three, or four. Half of Medicare costs right now occur in the last four years of life. This is the sort of flexibility feature which makes long-term uncertainties bearable. The proposal outline is simple: just use a portion of the earlier Medicare withholding tax to buy yourself the means to generate last-year-of-life costs. At the moment, that tax is 3% of income, half of which is contributed by the employer. Also at the moment, terminal care is about 25% of last-year costs, but it probably will eventually be over 50%, as the population ages and crowds death expectancy, not merely into Medicare, but into people older than 85.
That briefly sketches the proposal for Medicare -- phase it out gradually but voluntarily (as research eliminates the ten most expensive diseases). That offers a chance of more retirement funds if research science gets lucky, makes the choices always voluntary, and dangles retirement funds as an incentive. It's intended to be linked to first-year of life coverage, but the seeming impossibility of pre-funding newborns forces different approaches. Meanwhile, everybody alive has already been born, so there is less urgency. We take them up separately, and later integrate the two ends of life.
The graph is merely illustrative of the concept. Of course, we cannot predict stock market performance from past history, nor can we be sure inflation will continue at 3%. The point being made is the escrow concept allows part of the balance to remain untouched for early medical expenses but remains free to be released for designated ones, later. (The rest of the account balance has no such limitation, and thus is available for medical expenses.) The second point is the astonishing growth of a small amount of money if you give it time. And the final point is that you aren't going to get 7% passive return on your money unless you fight for it, even if you are investing in a stock market which has returned more than that for over a century. (The history of 1401(k) underlines the concern about intermediary fees). Right at the moment, the market is in one of its doldrums, but even in a booming market, you have to watch out for those fees. You can even hear it prophesied that the market will have a 2% total return for the next ten years. But that isn't what is important, what's important for this kind of thinking is What Will it Do, thirty years from now? And although no one can give an answer, it has been repeated many times that bull markets climb a wall of worry.
To return to the nitty-gritty, income could be further enhanced by extending the time period, compounding frequently, depositing earlier, and eliminating investment fees. In the background is the implication the depositor is well advised to be frugal in his early spending, pressuring his medical providers by being mindful of frugality, himself. Any action which pushes revenue toward the left (and away from the right) helps the customer put it to work with compound interest. The customer is always right, as John Wanamaker got rich by saying. Since the particular year, the subscriber was born will probably exert more influence over his retirement affluence than anything he can manipulate, he had better do what he can. And that is the basic argument for politically trying to extend the time period for compounding. At least on that issue, single-payer advocates have a point.
True, effective net income can also be increased by restraining inflation and/or middle-men lobbyists, but we are trying to make a larger point at the moment. We should aim the system time frame to be as long as possible, most easily achieved by linking programs (childhood, adulthood, and post-retirement) together. The only thing which needs to be continuously is the account into which money is deposited. There are significant disadvantages to bigness in organizations, so if you aren't going to compound the income, I'm not sure you are wise to advocate single-payer. Our first step would thus be, to try to include the time period covered by Medicare, since that's where most medical expense seems destined to originate in the future -- along with age 25-65 since that's when significant money is usually earned. Including any time period at all helps the math, but these two periods are particularly vital.
Originally published: Wednesday, May 25, 2016; most-recently modified: Monday, May 20, 2019