The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
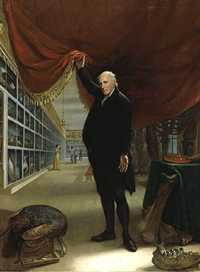
Charles Wilson Peale (1741-1827)
The Artist in His Museum
1822, Oil on canvas (The Joseph Harrison Jr. Collection)
Courtesy of the Pennsylvania Academy of
Fine Arts.
all of the red brick buildings on Independence Square look as though they were part of Independence Hall, but there is one exception. The building facing Fifth Street is Philosophical Hall, one of the four buildings of the American Philosophical Society. Right now, Philosophical Hall is used as a museum. It could be called the first museum in America, but not the oldest, because it had interruptions and different proprietorships. Charles Wilson Peale started his museum of curiosities there and then moved it to the second floor of Independence Hall, where he painted the famous portrait of himself holding up the curtain. In recent years, Philosophical Hall has again become a museum, holding treasures and curiosities belonging to the Philosophical Society itself. The docent is pleased to alternate between calling it America's new oldest museum, and America's oldest new museum. And, yes, the newell post has an Amity Button.
American Philosophical Society
Patents were established by the Constitution when it was a piece of parchment lying on a table fifty feet away from here, and the early patent office required the submission of a working model of every application for patent. After a while, that got to be a lot of working models lying around, and many of the more interesting ones are on display in the museum. Like the model of Fitch's first steamboat or the gadget Jefferson used, to make simultaneous copies of documents he was writing. That's right near the Gilbert Stuart copy of Washington's portrait, and von Neumann's first algorithm to be stored in his stored program machine, or computer, and Neil Armstrong's speech on the moon, concerning one step for mankind and all. It's a splendid museum, full of the real stuff, in a handsome Georgian building with sparkling immaculate marble staircases.
John Fitch received a US Patent for the Steamboat August 26, 1791
In the Eighteenth Century, Natural Philosophy was what we now call science. That's why PhDs get a degree of Doctor of Philosophy when they study chemistry and physics. The idea for forming a scientific society in America apparently originated with John Bartram. As so often happens, the originator couldn't quite get it established and had to call on Ben Franklin that impression of publicity, to get it off the ground. To be fair about it, Franklin was probably the more distinguished scientist of the two. To be even more fair about it, the organization struggled a bit until Thomas Jefferson (that's the one who was President of the United States) gave it a real publicity shove. During the depths of the 1930s depression, one of the members left it several million dollars with the stipulation that the investments should focus on common stock. Since buying stock in 1935 was widely regarded as about the stupidest thing an investor could do, this little episode reinforced a strong impression that membership in the APS is given to people who are very smart, not merely famous. The four buildings, the many fellowships, and the big endowment were largely made possible by this contraries investment decision.
There are eight hundred members, of whom 93 have won Nobel Prizes. Over the years, two hundred members have been awarded Nobel Prizes, but you must remember that the organization existed for 150 years before there was such a prize. Several U.S. Supreme Court justices are members and lots and lots of people who are famous. The docent comments that they look pretty much like everyone else. There's a rumor that Bill Gates turned down the offer of membership, so now we will just see. He's young enough to have several decades' opportunity to reconsider an offer, although the APS might just be old enough to lack interest in any second chances.
In their 1956 book "Philadelphia Scapple", Harold Donaldson Eberlein and Mrs. Henry Cadwalader give an interesting description of the evolution of the term "North of Market". In the early days of the city, almost all of the town was South of Market Street. In fact, an early 18th Century visitor once wrote that he always brought a fowling piece when he visited Philadelphia because the duck hunting was so good at the pond located at what is now 5th and Market.
When the Quaker meeting house was built at 4th and Arch Streets, many of the more important Quaker families thought it was important to build their houses nearby. In that way, Arch Street developed the reputation of being a Quaker Street. So the original meaning of the North of Market term was the Quaker ghetto. Quaker families continued to spread West along Arch Street or nearby, and this accounts for the location of the Friends Center at 15th and Cherry and related local activities. When the Free Quaker were evicted from the meeting at 4th and Arch because of their activities during the Revolution, they built their own meeting at -- 5th and Arch.
Chinese wall
During the Civil War, a number of people made fortunes that socially upscale people over in the Rittenhouse Square area considered disreputable, so elaborate but ostracized mansions marched due North up Broad Street, where they can still be observed as stranded whales in the slums, leaders without followers. The show houses of manufacturers of shoddy war goods soon gave the meaning of parvenu to the term North of Market.
And then, the Pennsylvania Railroad ran an elevated brick structure from 30th Street to City Hall Plaza, the so-called Chinese Wall. For nearly a century this ugly looming structure on Pennsylvania Boulevard, now John Kennedy Boulevard, with its smoky engines above, and dark dripping tunnels at street level, sliced the town in half and made it very unattractive to build or to live, North of Market. The Spring Garden area had some pretty large and expensive houses, but it was cut off by the railroad trestle and has only recently started to revive. It helped a lot to tear down the Chinese Wall, but that was fifty years ago, and the area has taken a long time to recover from the earlier diversion of social flow to the South of it. And, psychologically, North of Market will take even longer to recover from the implication of -- industrial slum.
center
Meanwhile, of course, Oriental immigration settled along Arch Street at 9th to 12th Streets, and we now have our Chinatown there, complete with street signs in oriental lettering. In effect, we have a real Chinese Wall, a social one. Just what will happen to this group is unclear, since it is readily observable that they like to cluster together, unlike the East Indian immigrants, who head for the suburbs as fast as they can. Since the Chinese colony is physically blocked on all sides by the Vine Street Expressway, the Convention Center, and the Ben Franklin Bridge, it is hard to know where they will flow if the group gets much larger. The depressed Vine Street crosstown expressway makes a definitive border for downtown, and the contrast between the two sides of this expressway is striking. On one side is Camelot, and on the other side, almost nothing is being built. The future of North of Market, at the moment, is a little unclear.
A silhouette map of the Hudson River from top to bottom shows several stretches of narrow river between several other wide stretches, almost like lakes. The narrows reflect the places where mountain ranges broke apart to let the river through, and the lakes are places where the water backed up until it got high enough to flow through the gorges. There's not much water pressure since the Hudson at the mouth of the river at New York Bay is only a few feet deeper than it is at Albany. Ben Franklin was the first to observe that the Hudson and Delaware are not exactly rivers; they are more like fjords, tidal up to Poughkeepsie and Marcus Hook, respectively. The Dutch had a settlement at New Amsterdam, of course, but there was another settlement around the Tappan Zee, and another cluster above West Point. Kingston was the dominant town of this upper settlement, but the British had burned it to the ground after their defeat at Saratoga in 1777. In 1782, Washington chose Newburgh to be his headquarters, where he remained for 16 months, the longest headquarters interval during the eight-year guerilla war.
Storm King Mountain
As always, Washington made excellent use of geography. The Storm King Mountain and West Point to its south narrowed the water route to New York down to a defensible defile. On the east side of the Hudson, the towering ridge not only protected the encampment from surprise but provided a lookout point at Beacon, where television towers now stand. The land is broken and semi-mountainous on the east side of the Hudson, all the way into Connecticut; an extension of difficult terrain which on the south crosses the Hudson and extends west into New Jersey. Reduced to its essentials, the British in New York and Washington in Newburgh were separated by a mountain range with a Hudson River water gap running through it. Immediately to the west beyond Newburgh however, the land is fairly flat until it rises to the watershed of Delaware. Washington could defend the Hudson against the British Navy at the narrows, eventually blocking the channel with a chain which was sufficient barrier to sailing vessels if they were vulnerable to cannon fire from the shore. If there was a land attack sweeping around behind Newburgh, Washington could escape by sailing up the Hudson; in that case, he would have boats and the pursuing British Army wouldn't. Such a daunting natural fortress was adequate for his situation since the British were equally reluctant to sustain casualties in frontal assaults so late in the war unless victory was fairly quick and easy. This was the general issue underlying the Benedict Arnold affair: blocking the British Navy from making a landing north of the watergap.
Battle of Yorktown
After the battle of Yorktown, the British could see there was no hope of subjugating large colonies using armies mostly supplied by sea. The Revolution settled down to attrition at sea, but the American privateers were winning that, too. Eventually, more British were lost to privateering than to warfare on land. The colonies were learning how to supply themselves with manufacturers, while the British were losing substantial amounts of trade with other parts of the Empire. Franklin in Paris was counting on Washington to maintain a credible threat; Washington was counting on Franklin to drive a hard bargain, but hurry up, please, our troops haven't been paid and are restless. The privateers were both suffering and inflicting appalling losses at sea, but their owners were getting rich. Most of the early great fortunes of Federalist America trace their origin to privateering. All of these emerging realities presented a bleak future to the British, and Franklin was masterful in rubbing it in. But if Washington lost control of his little army, a great deal more would be lost at the treaty negotiations.
Pierre Augustin Beaumarchais, the son of an 18th Century French watchmaker, was born Protestant in a Catholic country. While possibly inclined by this circumstance to be a free thinker, his unusual artfulness was more likely inborn. After revolutionizing watchmaking before he reached the age of twenty, with an escapement mechanism for small portable watches, he rose to social attention when the Royal Watchmaker claimed the invention was his own, and Beaumarchais sued him. Thus gaining Louis XV's notice, Beaumarchais became Royal Watchmaker himself. He was soon giving harp lessons to the ladies of the court, writing plays like The Barber of Seville, and engaging in business schemes with wealthy investors. His career as a court favorite lasted sixteen years, first bringing him considerable wealth, but then sudden ruination by a lurid lawsuit which cost him his fortune. In brief, Beaumarchais had tried to bribe a French judge with less money than his opponent offered, and so spent a few months in prison. After concluding a long, public battle through the appeals courts, he sought a more political role with the new young King, Louis XVI. He was sent to London to pay off a former French Agent, Chevalier D'Eon, who was blackmailing the French government. D'Eon's social connection to John Wilkes, the outspoken critic of the British King, sparked Beaumarchais' initial interest in Whig politics and the American rebellion.
John Wilkes
When he arrived in England Beaumarchais found British politics in turmoil; John Wilkes headed a whiggish opposition movement denouncing Royal authority and hosting gatherings of the like-minded, some of which Beaumarchais attended. Fueling these domestic British flames of liberal reform was the recent and increasingly serious rebellion on the other side of the Atlantic. As Beaumarchais spent more time in England discussing the rebellion with Virginian Arthur Lee (who highly exaggerated its strength), he became increasingly convinced it would be a good strategy for France to help the colonists. For all the trouble Arthur Lee ended up causing, he can fairly claim credit for enlisting Beaumarchais to French support for the American cause.
Charles Gravier, Comte de Vergennes
Beaumarchais reported his findings to Charles Gravier, Comte de Vergennes, the foreign minister of France. He urged the French government to support the American rebellion, consistently taking the line of French self-interest; after suffering a humiliating defeat in the Seven Year War, France might now undermine England's growing regional power by helping the colonists loosen their affiliation to the rising island empire.
When the young and hesitant Louis XVI finally agreed to take Beaumarchais' advice, it was still unclear whether the American rebellion was a serious movement. The French monarchy was not ready to unsettle its already shaky relationship with England by coming out in public support of untested rebels. To preserve the appearance of neutrality, the French Government loaned Beaumarchais one million lives in June 1776 to start a private trading firm, the Rodriguez Portales Company. This new firm would buy old French military supplies from the French government, then re-sell those supplies to the Americans with return payment of American products, primarily tobacco. Beaumarchais was therefore expected to run a completely self-sustaining operation, free from association with the French government. Rogue and adventurer that he was, Beaumarchais took on this risky challenge with enthusiasm, working tirelessly in France and around Europe to provide the Americans with ammunition, military supplies, and food. His efforts did not go undetected, however. England's ambassador to France, Lord Stormont, grew suspicious of Beaumarchais' frequent trips across the channel and notified the French government of his displeasure. But Beaumarchais simply ignored these protestations.
Matching Beaumarchais' work in establishing Rodrigez and Hortalez, the American Congress sent a covert representative to nurture French support. Silas Deane, sent to France under the disguise of a colonial merchant in July 1776, learned of Beaumarchais' plan to support the American army and at first, the two became fast friends. Unfortunately, this friendship sparked the jealousies of Colonists and Frenchmen alike. Arthur Lee became a particularly vicious opponent of the Beaumarchais/Deane pair, resenting Silas Deane for having been chosen over him as a diplomat to the French, and suspecting Beaumarchais of money laundering. Even when he was later sent in company with Benjamin Franklin to continue negotiations with France, Lee remained suspicious of Deane and Beaumarchais' collaboration. The American mission to France during this period remains famous for strife and factionalism, which was as much a free for all as two-sided animosity. Personal ambition and cultural differences complicated these relationships; no one eventually suffered more because of it than Beaumarchais and Deane.
While Deane negotiated with Beaumarchais, Arthur Lee corresponded with Congress to undermine both Beaumarchais and Silas Deane. Lee was highly suspicious of both men, accusing them of using the privateering scheme for their own profit. The result was a split in Congress between those who supported Lee and those who supported Deane's work with Beaumarchais. The first congress was full of alliances, tempers and faulty information that led to frequent, if not constant, conflict. The Lee brothers were particularly vocal opponents of an alliance with France, and this opposition by a prominent family within the Continental Congress kept French and American relations strained and hesitant.
The first shipment to the colonies by the Rodrigez and Hortalez Company carrying nearly 25,000 pounds of ammunition, was a shaky and often blind operation. Continental Congress never received news of Deane's plans (and request for ships) and remained busy working away at a proposed Declaration of Independence, the publication of which would, with luck, ensure France's official cooperation. Deane was forced to make crucial shipment decisions without the support or approval of Congress. Adding to this instability, the ships were discovered by Lord Stormont right before the first shipment left for the colonies, and the English Ambassador to France quickly protested their sailing to the French government. Vergennes, eager to keep smooth relations with England, particularly in view of the seeming failure of the American cause at that time, officially banned their sailing off the French coast. Fortunately for the Americans, Beaumarchais sent the supplies anyway, which were greeted warmly by colonists in Portsmouth, New Hampshire in early 1777. These supplies helped the colonists win the Battle of Saratoga, the success of which finally convinced the French to emerge in full support of the American Revolution. Beaumarchais continued to supply the Colonists despite England's protests, but privateering increased the threat of war between England and France.
Barber of Seville
By September 1777, Beaumarchais had shipped 5 million lives worth of supplies to America without repayment. By 1778 his firm had accrued so much debt that by the end of the war it was in complete ruin. The French government was unwilling to acknowledge its support for Beaumarchais before or after the war, and Silas Deane's entreaties were, unfortunately, not enough to convince Congress that the American colonies owed Beaumarchais for his generous work. Beaumarchais continued his requests for compensation after the war, and Congress continually refused or ignored these requests. Thirty-six years after his death, his heirs were paid back a small fraction of the original debt. Forced to travel to Congress to fight their ancestor's case, his descendants were awarded 800,000 lives of the several million owed. In effect, Beaumarchais nearly single-handedly supplied the American Revolution with arms receiving very little in return except his financial ruin.
It is surprising that a man with so much talent and character should have died in near obscurity; yet Beaumarchais' plays, not his political maneuverings, are what have survived today as part of the standard repertory. When his wildly successful The Barber of Seville premiered in 1775, Beaumarchais was already a well-known playwright and champion of the down-trodden common man. Perhaps he was too great for his own time; The Barber proved more popular when adapted into a libretto by Lorenzo Da Ponte and then later into an opera by Gioachino Rossini in 1814. An independent mind and flamboyant character immortalized his art, but the same characteristics may have brought him, and France, to political and financial ruin.
The Administrator of Fort Mifflin, Beth Beatty, recently addressed the Franklin Inn Club about it. The famous fort, whose defeat marked the end of Philadelphia's resistance to the British invasion, is now owned by the City of Philadelphia, hidden behind the approaches to the International Airport. It shows a lot of signs of two centuries of wear and tear because for a number of decades after the Revolution it was still in use as a fortification. Built on a swamp, one most notable feature is it can be very wet, much of the time, and is subject to repeated floods that most of us on the higher ground pass off as rainstorms. But it's still there, and it must be pretty sturdy.
British frigates were patrolling upper Delaware well before July 4, 1776, and Benjamin Franklin was a member of the Committee on Safety. As such, he is given credit for inventing the chevaux de frise, which filled in the gaps in the mudflats at the turn of the river. These inventions are best imagined as the "do not reverse" treadles of modern parking lots, buried in the riverbed and quite effectively preventing the sailing ships of the day from passing upstream. Fort Mercer was placed on a small bluff protecting the New Jersey side, and Fort Mifflin held the Pennsylvania side of the river, but more notably wallowing in the mud.
Fort Mifflin
The fort has been named after Thomas Mifflin, Pennsylvania's first governor. Unfortunately, Mifflin was the main conspirator in the so-called Conway Cabal which later tried to dislodge George Washington from the role of Commander while he was still at Valley Forge. Mifflin was a total drunkard, and behaved disgracefully as Governor, signing over huge plots of state land to himself, along with his subverted controller, John Nicholson. Much of the bankruptcy of Robert Morris can be traced to the manipulations of these two colonials, although that famous bankruptcy played such a central role in the political arguments of the early 19th Century it will probably always be difficult to be sure where to place blame. Since Morris was one of the three men (along with Franklin and Washington) without whom the Revolution could not have been won, his responsibility in the post-war land speculations tends to benefit from shifting the burden of proof toward the other two participants, perhaps even accurately.
Fort Mifflin Powder Room
An interesting part of the Fort Mifflin site is to discover that the powder magazines were buried underneath the foundation footings of the main brick defensive wall. The gunpowder effectively had a roof of the entire main wall. That made it particularly difficult for cannon fire to ignite the gunpowder stores and probably played a large role in the ability of the Fort to hold out against the British for considerably longer than anyone expected. Since the fort had been built while the British were still in control before the Revolution, the attackers were eventually able to consult with the architect, who advised them to bombard the Pennsylvania side of it, which was mainly made of mud rather than solid brick. It should be remembered that the British had disembarked at the Head of Elk in Maryland when they launched the original attack behind Philadelphia. They thus carried minimal supplies and food on what was mainly a cavalry charge, taking a great risk they would not be able to rejoin the British fleet in time. The fleet circled back down the Chesapeake Bay and returned up to the Eastern Maryland coast to Delaware Bay. When they found their way blocked for days and weeks at Fort Mifflin, Lord Howe's troops inside Philadelphia were at great risk of starving, and/or running out of ammunition. Washington seems to have recognized the advantages he had and was willing to sacrifice the fort for a prolonged defense. The British Navy on the downside of the Fort, equally aware of the need to break through quickly, pummelled the Fort with thousands of cannon shot and shell. The Americans inside the fort adopted the ingenious strategy of building the walls up at night, ready at dawn to withstand another day of bombardment. It has been reported that most of Ft. Mifflin's defenders were teen-aged boys, perhaps mostly overestimating the odds of their own survival.
It was a gallant try, but eventually the overwhelming force of the British Navy broke through. The American capital had been taken.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.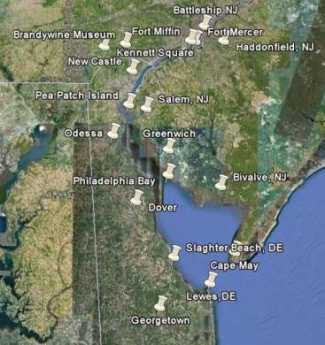 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.













{kind=link}