The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
MEETING OF THE SHAKSPERE SOCIETY OF PHILADELPHIA AT THE FRANKLIN INN CLUB ON OCTOBER 8, 2003
Secretary Peck in the chair. Other members present Ake, Bartlett, Bornemann, Cheston, Cramer, Fallon, Fisher, Friedman, Frye, Green, Griffin, Lehmann, Mabry, Madeira, O' Malley, Wheeler. Mr. Schmalzbach joined us as we began our reading of Macbeth.
Members joined in hearty praise of the Falstaffian Bard's birthday feast of last April hosted by Messrs. Friedman, Madeira, and Pope. Our hats are off to you, gentlemen!
The secretary has received two new email addresses from members; any others to be reported? Please let me know promptly if so. A reminder that notices of forthcoming meetings will be sent out only by email. If you wish to receive a telephone call as a reminder, please inform me: I will be happy to comply. Minutes too will be sent by email to those who are electronically up to date, and by regular mail to members who are still ensnared in snail status (so to speak).
We were sorry to hear that Edgar Scott, a member of very long standing, has decided to resign from the Society since he feels that he can no longer make the long drive home after dinner meetings.
We were reminded that the Philadelphia Shakespeare Festival is performing Julius Caesar until mid-November at its snug home on the second floor of the Lutheran Church parish building at 21st and Sansom streets. This group will stage As You Like It next February. Next March, People's Light and Theater Company in Malvern will also stage Caesar.
The Vice Dean announced that we will read Timon of Athens as soon as we finish Macbeth. Timon is not a play that most bookstores normally have in stock, so caveat emptor. Dr. Fallon mentioned how much he has enjoyed reading over the three parts of Henry VI recently. Margaret of Anjou is a particularly vivid character' and the only Shaksperian character to appear in four of the master's plays (Richard III as well as the three Sixes).
Col. Fallon asked us why the witches tempt Macbeth, and what their powers are: murky issues. They know the future, but they cannot harm the thane. How would the play be different without them? Is Macbeth a tool of the witches' in their power' or can he make moral choices? In early scenes, Macbeth is violent but virtuous, defending his king and country against invaders (Norwegians) and traitors (Cawdor). An Elizabethan audience would presumably have thought of contemporary events: the threat of invasion by powerful Spain over many years; local Roman Catholics ready to rebel against the Protestant queen whom the pope had urged them to overthrow; and the fear of civil war when Elizabeth dies only two or three years before this play was first performed.
Act One, Scene Three: Macbeth hears the bewitching promise of royal power. The seed of ambition is planted that Lady M. will force into early flower (as the gardeners among us might say). Macbeth is horrified to realize that as soon as the witches promise him a crown, he is thinking of murdering his way to power.
1.4'Lady Macbeth speaks in soliloquy about driving the morally squeamish Mac. to seize the throne. The Lady has a prominent role in only a few scenes, the Vice Dean reminded us; but what an impact she makes on readers and audiences! Local opera lovers will think of Lauren Flanigan's riveting incarnation of Lady M. last season in Verdi's version of the tale. Dr. Fallon pointed out that Lady Macbeth asks supernatural power to take away the feminine nature that gives her protection, customary in Elizabethan culture. Why does she collapse at the end of the play after showing such explosive strength of will in earlier scenes? Members spoke up vigorously on these and other issues about Lady M. and her influence on her spouse.
1.5'Lady Macbeth undermines Macbeth's moral qualms about killing his king, his kinsman, and his benefactor. Is she in effect her husband's alter ego, putting into powerful and seductive words the suppressed tempter's voice inside his own heart?
1.7'Macbeth argues with himself about the horror of killing his trusting royal cousin and then argues with his wife about the morality of the deed. By the end of his wonderful soliloquy, he seems certain to refuse to kill; but his wife's claim that he is not a man unless he seizes power by any means necessary quickly changes the direction of his thoughts: "Can we get away with it?" is all he asks. The Vice Dean reminded us of the frequent images of vulnerable children in this play. Macbeth refers to pity as a "naked newborn babe" in his soliloquy, his Lady tells him that she would smash the head of a suckling infant at her breast rather than refuse to be man enough to seize power; later, Lady Macduff's small child is murdered before her eyes by the thugs who kill her too. An infant's head appears to horrify Macbeth when the witches show him Banquo's royal progeny.
2.1'Macbeth is again powerfully smitten by conscience, as he shrinks in horror from a bloody dagger that his imagination holds before him. But he asks the stars to hide, the heavens to turn their eyes away as he goes to kill his king, like Tarquin the rapist going to violate vulnerable goodness.
OUR NEXT MEETING WILL BE ON OCTOBER 22, 2003. WE WILL BEGIN READING MACBETH AT ACT TWO, SCENE THREE.
Just about the cutest baseball park anywhere is Campbell's Field, best seen out the windows of the PATCO highspeed train as it crosses over the Ben Franklin Bridge into New Jersey. It's a regulation-size playing field with gleaming green grass, but comparatively small seating capacity. It's a great novelty to sit in the front row and have the umpire come over to chat, or to scold one of the players for spitting chewing tobacco. As told by Joel Seiden to the Right Angle Club, the performances of the home team Camden Riversharks is more about serious entertainment than serious baseball. On certain nights, there are fireworks, and free strawberry sundaes, and comedy. The finger food is cheap by professional sports standards, so it's a great place for dads to take their Little Leaguer sons.
About three-quarters of the audience usually come from New Jersey, and that's where team loyalty centers. There is hope that when the tramway to Pennsylvania finally gets built, or possibly the gambling casinos, more traffic will come over from Philadelphia. The greatest advertising comes from ordinary commuters, looking down from the bridge on a summer evening. A typical audience will be 3700 fans, rising to about 6000 on weekends.
Campbell Field
Although Campbell Field has a band-box new sparkle to it, it's had something of a bumpy financial history. It was built by Steve Schilling for $20 million with a promise to support yearly losses up to a million dollars annually. Unfortunately, he died young, leaving a will that prohibited further support, and sort of a tangled financial structure. As part of an effort to stimulate a Camden renewal, the Delaware River Port Authority loaned $8.5 million, Rutgers Camden owns the field, and Sovereign Bank put up a mortgage. Investor groups have expressed interest, Sovereign Bank has threatened foreclosure, and wrangles which have very little to do with baseball have dominated the private affairs of the team.
Because of the exemptions from antitrust which are exclusively available to organized baseball, no minor league team affiliated with a major league team may play within fifty miles of a major league team. Therefore, the Riversharks are an unaffiliated team, playing in the Atlantic League of Independents. However, this creates a source of revenue from selling promising players to major league scouts (Price: $5000). Since there is a top salary limit for players of $3000 a month, most players have a second job. They are professionals, but not exclusively professional. About 7 players are bought every year.
So, everybody involved struggles just a bit, but it adds to the gossip and buzz. So, take a trip on the PATCO train to the City Hall Station and walk three blocks, or take it to the Broadway Station and then the Riverline down to the field. Lots of fun.
Parson Weems, it seems, was a mercenary type who made up stories because he thought they would sell. Someone should explore the history of this anti-Weems debunking campaign for us, because it has distracted history from what may be a far more important truth about the founding, and the founder, of our country.
The address President Washington sent to his countrymen, published September 19, 1796, will apparently be forever referred to as his Farewell Address, and it is true that one of the important points he was making was the President should have only two terms of office, adding in his particular case the determination not to die while in office and create undesirable precedents for Presidential succession. It is also sometimes stressed that Washington cautioned the nation against all foreign entanglements, although likely he had in mind the particular conflicted loyalty at the time between England which we strongly resembled, and France to whom we owed a debt of gratitude for our independence. Surely he was telling the nation to watch out for its precarious independence, even at the price of disappointing old friends, and not really attempting to look centuries ahead in foreign relations. The point about a third term was a pretty firm one; Washington's greatest achievement in the eyes of the world was to renounce all resemblance to monarchy, which he could have had for the asking.
Farewell Address for George Washington
Much deeper meaning for the address is suggested when you search, let's say with Google, for the origins of the speech's repeated maxim, Honesty is the best policy. It sounds like the sort of thing Ben Franklin would put in his Almanac, but didn't. There are even times in Franklin's life when it might be questioned whether he really believed honesty was always the best choice for every situation, and Franklin's true belief might possibly have been closer to advising that you should strive to avoid getting caught misleading people. The opinion that honesty is the best policy sounds as if it might come from Shakespeare, or Cervante's Don Quixote; something pretty close can be found in both places. It might be much older than that; the phrase and a detailed examination of its merits can be found in the works of Quintilian, 69 AD. George Washington was unlikely to have read any classical Roman essays, but James Madison the favorite student of John Witherspoon at Princeton might well have been familiar with Quintilian. But these stray remarks about honesty are merely scatterings over fifteen centuries, mostly throw-away lines. It is only in the last decades of the Eighteenth Century that the little maxim is found peppered in the speeches of many people, beginning to use it as a cliche to adorn some other point of emphasis.
It is our true policy to steer clear of permanent alliances with any portion of the foreign world; so far, I mean, as we are now at liberty to do it; for let me not be understood as capable of patronizing infidelity to existing engagements. I hold the maxim no less applicable to public than to private affairs, that honesty is always the best policy. I repeat it, therefore, let those engagements be observed in their genuine sense. But, in my opinion, it is unnecessary and would be unwise to extend them.
The point begins to catch the imagination that perhaps this flowering of a maxim can be traced to Washington's Farewell Address. It's unlikely that George Washington actually coined the phrase that honesty was the best policy, any more than Franklin Roosevelt coined the motto that all we have to fear is fear itself, or John Kennedy originated the happy phrase that we should ask not what our country can do for us, etc. Our more sophisticated views of Presidential rhetoric are now quite broad enough to accept the existence of ghostwriters and wordsmiths. It is current practice to agree that credit for originating a phrase adheres rightly to the person symbolized later when the phrase enters common parlance. To think otherwise is to become entangled in bickering about who wrote Shakespeare's plays, or who really wrote the various books of the Bible.
President's House Philadelphia
There is, however, historical importance to the speech-writer question in Washington's case. We are told that Washington had asked James Madison to draw up a speech for the occasion of his declining to accept a second term of office in 1792, but the whole matter was reconsidered when various advisors finally persuaded the President that the country needed him at the helm for more than four years. The speech was therefore set aside but revised and re-issued four years later. By this time, however, Washington and Madison had experienced their fateful falling-out, and therefore Madison's arch-enemy Alexander Hamilton did the re-writing. That honesty is the best policy should survive as a centerpiece in an address co-edited by such bitter philosophical enemies, plus some passing reflection on the personalities of the three men, should suffice to dispel most doubt that the sentiment was Washington's and that it must have been held very intensely by him. Madison may well have planted it, and he might very well have got it in turn from Cervantes or Quintilian. David Hume of Scotland might be an even likelier source. But overall it is hard to let go of the idea that Washington seized on it as a summary of something he fiercely believed.
There are differing degrees of and situations for honesty, of course; surely the most trivial is the sort of honesty Parson Weems was imagining in the little lad who would become our greatest leader. It really is not necessary to believe the courage to risk a whipping by a schoolboy is a core value which evolves into the broad economic vision for a nation. The legal profession, for example, may even overvalue absolute precision of wording, sometimes tolerating exquisite accuracy which artfully avoids full disclosure, caveat emptor. The military academies come closer to Washington's meaning by stressing to their graduates that what matters is not what is said, but what is communicated. At the time of the Farewell letter, what agitated Washington most was political partisanship -- political parties -- and overzealous effort to defeat the opinions of honest opponents rather than strive for a resolution of problems by bargain and compromise. In his youth, Washington was a surveyor, deeply impressed by the advantages of getting things straight the first time. Washington was to lose the argument over political parties, but while this defeat was among his greatest disappointments, his resistance still shines like a beacon.
It is hard to discern whether Washington had the depth of economic insight to emphasize the feature of honesty is the best policy which has the greatest importance to the Twenty-first Century. However, it is possible he did, because he was speaking in the midst of Quaker Philadelphia, having centered most of his public life there. Puritan Boston deeply believed that God had commanded honesty in His followers, honesty for its own sake, and the sake of the honest person's soul. But the wealth of Boston was overshadowed by thriving Eighteenth-century Quaker Philadelphia. Honesty to a Quaker was, of course, a good thing in itself, but experience showed that strict honesty in commercial dealings, and friendliness in all dealings, was very good for business. And conversely, the example of success on all sides encourages others to be honest and friendly when perhaps it was not their first inclination; honesty is catching. John Adams was scornful of those who do the right thing for the wrong reason, but this viewpoint gets ignored in the Twenty-first century. What is important for the third world to grasp is not intuitively obvious; they see abundant examples of getting rich at the expense of others, so much so that the third world and much of our own is willing to believe that if you have prospered, you must have stolen. If the third world cannot grasp the higher truth, we despair of ever getting along with them. Indeed, we may need to worry about skeptics increasing in our own midst. If Washington ever wavered, however, no one has told us of it.
A popular legend of our founding fathers depicts a sudden 18th Century flowering of talent, even genius, establishing a new nation. More recently, historians have searched for personal material about the individual founders, humanizing them with warts, so to speak. A question nevertheless arises how a nation with the present population of Detroit could produce such outstanding leadership in what was then a scattered colonial frontier region. Men, that is. In our legends, the founders were all men.
Long before the feminist movement gathered momentum, historians like Rufus Wilmot Griswold and Abigail Adams Smith had chronicled the impact of the high society of George Washington's term of office as president, which was in part a conscious effort by Washington to show the new republic to the world, cutting just as fine a figure as the nations of old Europe. Martha Washington, soon called Lady Washington, was an uncomfortable central figure in the new social scene, and her dismay at being the President's wife, her anxiousness to retire from prominence as soon as his term was over, suggest the idea for a Republican Court probably did not start with her. Elizabeth Schuyler Hamilton, Alexander Hamilton's wife, might seem more likely but the real originator is not known. For present purposes, a plausible theory is that soldier George Washington and bachelor James Madison had the concept but couldn't pull it off; and then some determined ladies of the court soon showed them all, what was what.
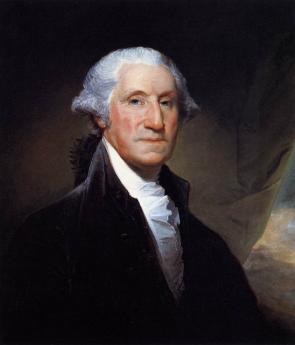
George Washington
George Washington began the process by instituting formal receptions for visiting males and Martha cooperated by holding Friday evening receptions, at which she was introduced to the wives of important political figures. The regular weekly events of the Presidency soon consisted of a reception by George Washington for new foreign ambassadors and other important foreign visitors, with a formal state dinner with a politically balanced invitation list on Thursday evening, and Lady Washington's reception on Friday with primarily a social purpose, leaning somewhat in the direction of letting the wives of important politicians shine in the social limelight. While the receptions were usually conducted with scripted formality, some notable exceptions were thought worthy of comment. Over twenty years earlier, Washington at Valley Forge had danced for three hours with Cathy Greene, the wife of Nathaniel Greene. When the widow Greene passed through one of the much later presidential levees, Washington suddenly bent over and kissed her, as "an impromptu act of spontaneity." The effect of the levees was to unite the elites of wealth and power, coming to Philadelphia from all thirteen colonies, now risen to statehood. Plantation owners from the South, ship owners, and merchants from the North met the daughters of socially prominent families and quite frequently married them. A courteous and civilized environment unified the new nation at its pinnacle by having local leaders mixing with other local leaders, becoming national leaders in the process. A politician in this new nation could rise to being someone of consequence socially. To be skillful in the social graces, particularly if there was wealth associated, was to advance in politics; to be boorish or loutish was to drop down somewhat in the scale of political influence, slowly but surely losing power to those who did have such graces. Put a backwoods politician into new formal clothes, force him to behave in an unaccustomed way in the midst of those more skillful at it, enlist the fearsome pressure of his ambitious wife to shine in the spotlight; and the fear of looking foolish soon enough pushes him toward conformity.
Anne Willing Bingham
After the first year, then the developing Republican Court. Martha Washington, of course, had her own mansion at Mount Vernon, but
Anne Bingham had one within easy walking distance of Independence Hall. The Wife of the richest man in America, Anne Willing Bingham was the daughter of Thomas Willing the head of the most prominent merchant family in Philadelphia. Anne's husband William Bingham had achieved richest-man status at the age of 28 (by running a large privateer fleet in the Caribbean)and was not only able to build a splendid mansion patterned after that of a London aristocrat at 3rd an Spruce Streets,but had taken his young and beautiful wife on an extensive tour of the royal courts of Europe which lasted several years. It is said that Robert Morris later contributed to his own bankruptcy by attempting to match the Bingham mansion with a Morris mansion at 7th and Market, which had to be torn down for lack of money before it was completed. Since most of the wealthy hostesses attempting to achieve prominence in the newly forming Court had never been to Europe, there was no choice but to accept the judgment of Mrs. Bingham in such matters, especially since she had the biggest showplace in town. While the truth of a story about her is uncertain, it accurately illustrates the flavor of the social atmosphere that it could be said that the Dauphin, heir to the throne of France, once went to her father to request her sister's hand in marriage. The young prince was then living in exile at 4th and Locust, in temporarily impoverished circumstances. Old Tom Willing, as the story goes, said No. "If you do not become the King of France, you will be no match for her. And if you do become the King, she will be no match for you."
It does seem to be true almost every prominent lady in the Republican Court was described by contemporaries as astonishingly beautiful, but at least in the case of Anne Willing Bingham, her surviving portraits support this description. John Adams, who had his brilliant wife Abigail for comparison, was overwhelmed by Mrs. Bingham's ability to hold her own on political subjects at the dinner table. And George Washington, who loved to dance with the prettiest lady available, greatly favored Anne as a partner. In time, she asserted herself to the extent of pestering Washington into having his portrait painted by Gilbert Stuart when the painter was in town. Washington ordinarily disliked having his pictures painted, avoiding it when he could. There are nevertheless a great many pictures of Washington on display, crossing the Delaware and whatnot, all showing the same grim face. After his death, it became necessary for most of the many new pictures of him to attach the same Gilbert Stuart head to a variety of imaginary depictions. Benjamin Franklin, by contrast, seemed to enjoy the experience of being a sitter so there are many more portraits of him actually drawn fro life. Add Washington's social sponsorship an almost unlimited personal budget for parties, and Anne Bingham quickly established herself as the reigning queen of the court without even provoking Martha Washington's hostility. This was a busy ladies' world; one new arrival in Philadelphia described herself as exhausted by having to return the courtesy visits of ninety different ladies during her early weeks in town. The expense of such competition emerges from brief reflection on the variety of clothes needed to keep up with changing styles, and the elegance of carriages, footmen, etc.
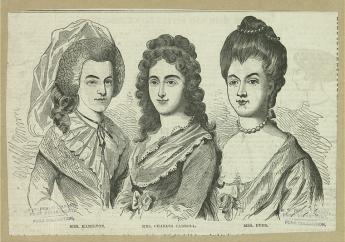
The Chew Sisters
Anne Willing Bingham was soon joined at the center of things by two Chew sisters, naturally referred to as astonishingly beautiful, who not only had their own mansions, but also Cliveden the summer place in Germantown as available venues for parties. It was commonly stated to be "social suicide, not to be home when the Chew sisters came to call." Delicious gossip was, of course, a strong undercurrent in such a social whirl, and Harriet Chew Carroll made a significant contribution. This daughter of Benjamin Chew the former Chief Justice (and Son of William Penn's personal lawyer)had married the son of very rich Charles Carroll of Carrollton, Maryland, but had to drop out of society because of notoriety associated with her abusively alcoholic husband. Similarly, Catherine Alexander Duer, who had married the son of the New Jersey patriot Lord Stirling, lost her social standing when her husband got deeply into debt in ventures with Robert Morris to the tune of today's equivalent of $40 million. As a Treasury official, there was a question of Duer's using public money to speculate privately, although he died in debtors prison before matters were completely clarified. His wife, who was known for having fifteen different wines on the dinner table, ended up her days running a boarding home to support herself. No doubt other transgressions were suppressed or covered up, while the political process was sufficiently advanced even in the early days of the Republic, to introduce some deliberate falsehood into the gossip mill. No doubt, one of the strongest drinks at the receptions was the bubbly wine of knowing all the inside scoop. And meanwhile, the potential disgrace of falling from favor was immensely powerful in enforcing conformity among those who might otherwise think themselves immune to it.
Some People were left out for various reasons, even if they could keep up financially or politically. It's always a little hard to identify why some people are social duds. Abigail Adams Smith seems to have been one of these, a constant source of adverse commentary about the extravagance, hypocrisy, etc., etc. English literature at this time has Jane Austen and William Makepeace Thackery, Pope Swift, and Dr. Johnson to satirize and constrain the social whirl, but American seems to have produced little more than correspondence and hushed remarks. The feeling of resentment was constantly growing in Republican circles, however, feeding a growing undercurrent of hostility undermining something so elitist and therefore somehow UnAmerican. After ten years in Philadelphia elegance, the District of Columbia was discovered to be scarcely more than a dismal swamp when the capital moved there, a place quite unsuited to high society. Dolley Madison revived things somewhat while acting as hostess for the widower Thomas Jefferson, and when her husband became the next President, opened her receptions to the general public. One can easily imagine the intense hostility of Andrew Jackson to any of this, however. Washington DC has since evolved a pallid political social whirl because America still has politically ambitious rich folks and plenty of money for indirect lobbying. But it hasn't ever been the same as the glory days in Philadelphia, and probably never will be. Present members of the financial/political elite who now work in Washington are in a great hurry to leave town every weekend, abandoning its empty office building to the tourists and civil servants.
The Republican Court
The Republican Court served an important role in helping America unify thirteen colonies into a single nation. Because Philadelphia was for a time the center of the country, economically, socially and politically, all people of prominence in here, wanted to know each other. Variations of wealth and breeding stratified the women somewhat differently from the Variations of wealth and power of their husbands, ad constant mixing of the two strata unified the leadership of the new nation in ways that would have developed more slowly without it. The forced conversations of the receptions stratified independently but helped all the newcomers to the scene to adapt to the realities more comfortably. Each group, private and public watched a constant parade of aggressive climbers sort themselves out and searched for how they had made out; wealth got you to the top in one group, private and public, watched a constant parade of aggressive climbers sort themselves out and searched for how they had made out; wealth got you to the top in one group, power got you there in the other. But in both groups, the cruelties of social striving made the iron rule clear that such things as wit, gracefulness, physical attractiveness, education and breeding were qualities that floated you to the top of the soup of any flavor. When you are forming a new nation, perceptions of that sort are important to acknowledge. The American aristocracy could be circumvented among the many ways to the top, could be sneered at by those who lacked its unattainable features, and could be sniggered at by real aristocrats of real aristocracies in Old Europe. But it served well enough as a role model for a constant stream of new immigrants, and set a pattern for new communities of the interior, also seeking a sense of cultural direction. Like the breeding of horses and dogs that is such a constant upper-class avocation, there is a genetic message, too. Rich men marry beautiful women, so their children or grandchildren tend to be handsome. Handsome or not, gracefulness in social circles is learned at home. Darwin teaches you one thing, Adam Smith's hidden hand teaches another; both are worth attending to. Given eight or ten generations, this sort of evolutionary pressure forms a community, then a nation. It has certainly left major imprint on Philadelphia.
Abigail Adams Smith
On the rest of the nation as well, but in different ways. Along the East Coast, first families tend to persist and went to school so to speak in Philadelphia during Washington's presidency. Mary Ann Goodrich was a witty and Wealthy wife of a Connecticut political leader. Elizabeth Schuyler Hamilton was the famously vivacious wife of Alexander Hamilton of New York. Alice De Lancey Izard was the toast of Charleston, South Carolina. Patsy Jefferson Married Thomas Randolph of Virginia. Mary White Morris of Philadelphia had a bumpy trip as the wife of Robert Morris. In East Coast high society, the ladies usually have middle names.
Over three centuries, three main streams of immigrants plodded their way across the continent to the West and then merged. There were westward pioneers from north of Philadelphia with a certain kind of accent, from South of Philadelphia with another, and from Philadelphia with the normal way of talking. Each of them was following role models within its own cultural pattern, but the significance of middle names is now only a tip-off to insiders. There are patches of country, like Appalachia we are Texas, which brush off any allegiance to distant origins. But to the degree we are unified, the Philadelphia mixing bowl of the Social Scene during George Washington's presidency is a big part of how we got that way.
Pierre Augustin Beaumarchais, the son of an 18th Century French watchmaker, was born Protestant in a Catholic country. While possibly inclined by this circumstance to be a free thinker, his unusual artfulness was more likely inborn. After revolutionizing watchmaking before he reached the age of twenty, with an escapement mechanism for small portable watches, he rose to social attention when the Royal Watchmaker claimed the invention was his own, and Beaumarchais sued him. Thus gaining Louis XV's notice, Beaumarchais became Royal Watchmaker himself. He was soon giving harp lessons to the ladies of the court, writing plays like The Barber of Seville, and engaging in business schemes with wealthy investors. His career as a court favorite lasted sixteen years, first bringing him considerable wealth, but then sudden ruination by a lurid lawsuit which cost him his fortune. In brief, Beaumarchais had tried to bribe a French judge with less money than his opponent offered, and so spent a few months in prison. After concluding a long, public battle through the appeals courts, he sought a more political role with the new young King, Louis XVI. He was sent to London to pay off a former French Agent, Chevalier D'Eon, who was blackmailing the French government. D'Eon's social connection to John Wilkes, the outspoken critic of the British King, sparked Beaumarchais' initial interest in Whig politics and the American rebellion.
John Wilkes
When he arrived in England Beaumarchais found British politics in turmoil; John Wilkes headed a whiggish opposition movement denouncing Royal authority and hosting gatherings of the like-minded, some of which Beaumarchais attended. Fueling these domestic British flames of liberal reform was the recent and increasingly serious rebellion on the other side of the Atlantic. As Beaumarchais spent more time in England discussing the rebellion with Virginian Arthur Lee (who highly exaggerated its strength), he became increasingly convinced it would be a good strategy for France to help the colonists. For all the trouble Arthur Lee ended up causing, he can fairly claim credit for enlisting Beaumarchais to French support for the American cause.
Charles Gravier, Comte de Vergennes
Beaumarchais reported his findings to Charles Gravier, Comte de Vergennes, the foreign minister of France. He urged the French government to support the American rebellion, consistently taking the line of French self-interest; after suffering a humiliating defeat in the Seven Year War, France might now undermine England's growing regional power by helping the colonists loosen their affiliation to the rising island empire.
When the young and hesitant Louis XVI finally agreed to take Beaumarchais' advice, it was still unclear whether the American rebellion was a serious movement. The French monarchy was not ready to unsettle its already shaky relationship with England by coming out in public support of untested rebels. To preserve the appearance of neutrality, the French Government loaned Beaumarchais one million lives in June 1776 to start a private trading firm, the Rodriguez Portales Company. This new firm would buy old French military supplies from the French government, then re-sell those supplies to the Americans with return payment of American products, primarily tobacco. Beaumarchais was therefore expected to run a completely self-sustaining operation, free from association with the French government. Rogue and adventurer that he was, Beaumarchais took on this risky challenge with enthusiasm, working tirelessly in France and around Europe to provide the Americans with ammunition, military supplies, and food. His efforts did not go undetected, however. England's ambassador to France, Lord Stormont, grew suspicious of Beaumarchais' frequent trips across the channel and notified the French government of his displeasure. But Beaumarchais simply ignored these protestations.
Matching Beaumarchais' work in establishing Rodrigez and Hortalez, the American Congress sent a covert representative to nurture French support. Silas Deane, sent to France under the disguise of a colonial merchant in July 1776, learned of Beaumarchais' plan to support the American army and at first, the two became fast friends. Unfortunately, this friendship sparked the jealousies of Colonists and Frenchmen alike. Arthur Lee became a particularly vicious opponent of the Beaumarchais/Deane pair, resenting Silas Deane for having been chosen over him as a diplomat to the French, and suspecting Beaumarchais of money laundering. Even when he was later sent in company with Benjamin Franklin to continue negotiations with France, Lee remained suspicious of Deane and Beaumarchais' collaboration. The American mission to France during this period remains famous for strife and factionalism, which was as much a free for all as two-sided animosity. Personal ambition and cultural differences complicated these relationships; no one eventually suffered more because of it than Beaumarchais and Deane.
While Deane negotiated with Beaumarchais, Arthur Lee corresponded with Congress to undermine both Beaumarchais and Silas Deane. Lee was highly suspicious of both men, accusing them of using the privateering scheme for their own profit. The result was a split in Congress between those who supported Lee and those who supported Deane's work with Beaumarchais. The first congress was full of alliances, tempers and faulty information that led to frequent, if not constant, conflict. The Lee brothers were particularly vocal opponents of an alliance with France, and this opposition by a prominent family within the Continental Congress kept French and American relations strained and hesitant.
The first shipment to the colonies by the Rodrigez and Hortalez Company carrying nearly 25,000 pounds of ammunition, was a shaky and often blind operation. Continental Congress never received news of Deane's plans (and request for ships) and remained busy working away at a proposed Declaration of Independence, the publication of which would, with luck, ensure France's official cooperation. Deane was forced to make crucial shipment decisions without the support or approval of Congress. Adding to this instability, the ships were discovered by Lord Stormont right before the first shipment left for the colonies, and the English Ambassador to France quickly protested their sailing to the French government. Vergennes, eager to keep smooth relations with England, particularly in view of the seeming failure of the American cause at that time, officially banned their sailing off the French coast. Fortunately for the Americans, Beaumarchais sent the supplies anyway, which were greeted warmly by colonists in Portsmouth, New Hampshire in early 1777. These supplies helped the colonists win the Battle of Saratoga, the success of which finally convinced the French to emerge in full support of the American Revolution. Beaumarchais continued to supply the Colonists despite England's protests, but privateering increased the threat of war between England and France.
Barber of Seville
By September 1777, Beaumarchais had shipped 5 million lives worth of supplies to America without repayment. By 1778 his firm had accrued so much debt that by the end of the war it was in complete ruin. The French government was unwilling to acknowledge its support for Beaumarchais before or after the war, and Silas Deane's entreaties were, unfortunately, not enough to convince Congress that the American colonies owed Beaumarchais for his generous work. Beaumarchais continued his requests for compensation after the war, and Congress continually refused or ignored these requests. Thirty-six years after his death, his heirs were paid back a small fraction of the original debt. Forced to travel to Congress to fight their ancestor's case, his descendants were awarded 800,000 lives of the several million owed. In effect, Beaumarchais nearly single-handedly supplied the American Revolution with arms receiving very little in return except his financial ruin.
It is surprising that a man with so much talent and character should have died in near obscurity; yet Beaumarchais' plays, not his political maneuverings, are what have survived today as part of the standard repertory. When his wildly successful The Barber of Seville premiered in 1775, Beaumarchais was already a well-known playwright and champion of the down-trodden common man. Perhaps he was too great for his own time; The Barber proved more popular when adapted into a libretto by Lorenzo Da Ponte and then later into an opera by Gioachino Rossini in 1814. An independent mind and flamboyant character immortalized his art, but the same characteristics may have brought him, and France, to political and financial ruin.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.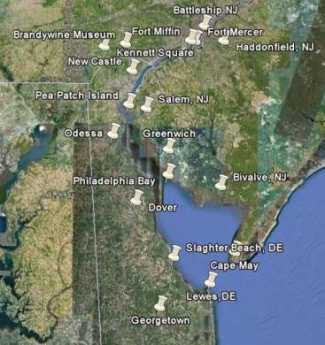 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.